Brain Stroke treatment
Reading File
Finding Sources
Searching PubMed
"stroke" AND "treatment" AND "guidelines"
Searching Images
ischemic stroke treatment thrombolysis thrombectomy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ischemic stroke" AND "mechanical thrombectomy"
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I have rich, comprehensive content across all major stroke treatment domains. Now I'll compile the full answer.
Brain Stroke: Treatment
Stroke treatment depends critically on type (ischemic vs. hemorrhagic), time from onset, and stroke severity. Approximately 85% of strokes are ischemic; the remainder are hemorrhagic (intracerebral hemorrhage [ICH] ~10–15%, subarachnoid hemorrhage [SAH] ~5%).
1. Initial Emergency Assessment
"Time is Brain" — ~1.9 million neurons die every minute during a major stroke.
- Immediate non-contrast CT head to exclude hemorrhage before any thrombolytic therapy
- CT/MR angiography to detect large vessel occlusion (LVO)
- CT perfusion (CTP) or diffusion/FLAIR MRI if wake-up or unknown-onset stroke
- NIHSS score, glucose, coagulation studies, renal function
- Blood pressure must be stabilized before intervention
2. Ischemic Stroke Treatment
A. IV Thrombolysis (tPA)
The cornerstone of acute ischemic stroke therapy since 1996.
Alteplase
- Dose: 0.9 mg/kg IV (max 90 mg); 10% as bolus over 1 minute, remainder over 60 minutes
- Time window: Within 3 hours (FDA-approved); can be extended to 4.5 hours for selected patients (ECASS III criteria)
- Evidence base: NINDS trial (landmark RCT showing improved outcomes vs. placebo)
- Low-dose alteplase (0.6 mg/kg) was shown noninferior to standard dose in Asian populations (ENCHANTED trial), with fewer hemorrhagic complications
Tenecteplase
- A newer tPA with greater fibrin specificity and longer half-life, administered as a single IV bolus (0.25 mg/kg, max 25 mg)
- A 2024 systematic review & meta-analysis (PMID 39413337) confirmed tenecteplase is non-inferior to alteplase within 4.5 hours and offers practical advantages over alteplase
- Guidelines now recognize tenecteplase as an acceptable alternative
Extended window thrombolysis (>4.5 hours)
- A 2025 meta-analysis (PMID 39882605) supports thrombolysis beyond 4.5 hours in carefully selected patients using imaging mismatch criteria (DWI-FLAIR mismatch for wake-up stroke; perfusion mismatch for late presentation)
- DWI-FLAIR mismatch (positive DWI, negative FLAIR) indicates stroke is likely <4.5 hours old and may guide treatment decisions in unknown-onset cases
Key contraindications to thrombolysis:
- Active intracranial hemorrhage on CT
- Recent major surgery/trauma (<14 days)
- SBP >185 / DBP >110 mmHg (uncontrolled)
- INR >1.7 or prior anticoagulation with recent dosing (depends on agent)
- Platelet count <100,000
- Prior stroke + diabetes combination
- Mild non-disabling stroke (NIHSS 0–5, nondisabling): not recommended (PRISMS trial)
- Mild but disabling stroke: alteplase is recommended within 3–4.5 hours
Blood pressure management during/after thrombolysis:
| BP Level | Treatment |
|---|---|
| SBP 180–230 / DBP 105–120 mmHg | Labetalol 10 mg IV q10–20 min (max 300 mg) or infusion 2–8 mg/min |
| SBP >230 / DBP 121–140 mmHg | Labetalol 10 mg IV + infusion, or Nicardipine 5–15 mg/h infusion; consider sodium nitroprusside if refractory |
Monitor BP every 15 minutes during infusion, then every 30 minutes for 6 hours, then hourly for 16 hours. (Rosen's Emergency Medicine, AHA/ASA 2019 guidelines)
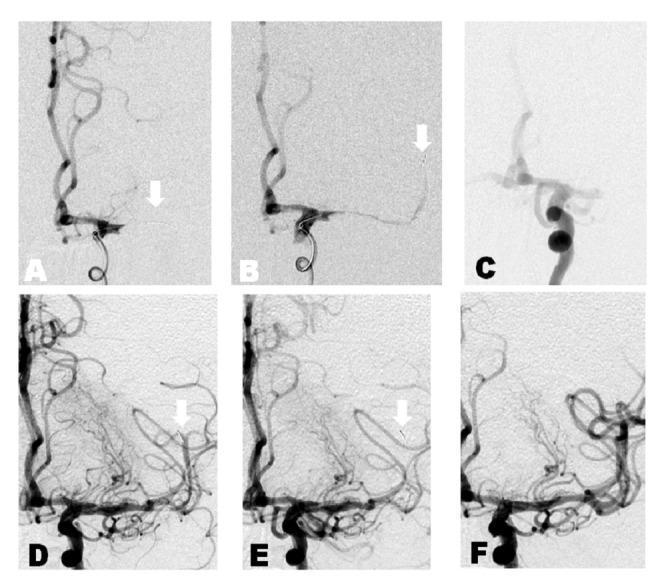
B. Mechanical Thrombectomy (Endovascular)
A major breakthrough: new-generation stent retriever devices proved definitively effective in 2015 (MR CLEAN, ESCAPE, EXTEND-IA, SWIFT PRIME, REVASCAT, THRACE trials).
Indications (0–6 hours):
- Age ≥18
- Large vessel occlusion: ICA or M1 segment of MCA
- NIHSS ≥6
- ASPECTS ≥6 (adequate viable brain)
- No significant prestroke disability (mRS ≤1)
- Can be combined with IV alteplase if eligible
Extended window (6–16 hours): DAWN and DEFUSE 3 criteria — CT perfusion or DWI mismatch required:
- Core infarct ≤70 mL, mismatch volume ≥15 mL, mismatch ratio ≥1.8
Extended window (16–24 hours): DAWN criteria — core ≤30 mL (age <80) or ≤20 mL (age ≥80); NIHSS ≥10 if 16–24 h from last seen well. DAWN trial showed mRS 0–2 at 90 days of 49% vs. 13% with standard care.
Key outcomes: Each 1-hour delay reduces odds of functional independence; benefit nonsignificant after 7 hours in pooled data. Achieves TICI Grade 3 (complete reperfusion) when successful.
C. Supportive Medical Management (Ischemic)
| Parameter | Target |
|---|---|
| Blood glucose | 140–180 mg/dL; treat hypoglycemia (<60 mg/dL) with IV dextrose |
| Temperature | Normothermia (fever worsens outcomes) |
| Antiplatelet (non-thrombolysis eligible) | Aspirin 325 mg within 24–48 h; reduce to 81 mg post-acute |
| Anticoagulation | NOT routine for acute ischemic stroke; indicated for atrial fibrillation (start after 4–14 days with DOAC or warfarin) |
3. Hemorrhagic Stroke Treatment
A. Intracerebral Hemorrhage (ICH)
ICH constitutes ~10–20% of strokes with ~50% 30-day mortality. Main causes: hypertension (72–81%), cerebral amyloid angiopathy, anticoagulant use. (Bradley & Daroff's Neurology)
Acute management:
| Priority | Intervention |
|---|---|
| Blood pressure | Rapid lowering to SBP <140 mmHg reduces hematoma expansion (ATACH-2 / INTERACT2 evidence) |
| ICP management | Head elevation 30°, osmotic therapy (mannitol/hypertonic saline), avoid hypoxia/hypercapnia |
| Coagulopathy reversal | Vitamin K antagonist → 4-factor PCC + vitamin K; Dabigatran → idarucizumab; Factor Xa inhibitors → andexanet alfa; Heparin → protamine sulfate |
| Platelet transfusion | For patients on antiplatelet agents with life-threatening ICH and thrombocytopenia |
Surgical management:
- Surgical hematoma evacuation is controversial — generally indicated for:
- Cerebellar hemorrhage >3 cm causing brainstem compression or hydrocephalus (urgent neurosurgical intervention)
- Lobar ICH with neurological deterioration
- Deep/basal ganglia ICH: surgery generally not beneficial (STICH trials)
- Hemicraniectomy for large hemispheric infarcts with malignant edema
Long-term prevention after ICH:
- Target BP <130/80 mmHg
- Antiplatelet resumption: RESTART trial showed antiplatelet therapy after ICH did not increase recurrent hemorrhage and reduced composite vascular events by 35%
- Oral anticoagulation after ICH with atrial fibrillation: observational registries suggest benefit; decision individualized; typically delayed ≥4–8 weeks
B. Subarachnoid Hemorrhage (SAH)
- Nimodipine (calcium channel blocker) 60 mg every 4 hours for 21 days — reduces cerebral vasospasm-related infarction (strong evidence)
- Urgent neurosurgical clipping or endovascular coiling of ruptured aneurysm
- Ventricular drainage for hydrocephalus
4. Secondary Stroke Prevention
| Mechanism | Agent |
|---|---|
| Non-cardioembolic ischemic stroke/TIA | Aspirin 81–325 mg/day or clopidogrel or aspirin + dipyridamole (latter two superior to aspirin alone) |
| High-risk TIA / minor stroke (POINT/CHANCE) | Short-term DAPT (aspirin + clopidogrel ×21 days), then single antiplatelet |
| Cardioembolic (atrial fibrillation) | DOAC (preferred) or warfarin (INR 2–3) |
| Carotid stenosis 70–99% (symptomatic) | Carotid endarterectomy (CEA) ± carotid artery stenting (CREST trial: equal efficacy, higher periprocedural stroke risk with stenting) |
| Asymptomatic carotid stenosis ≥60% | CEA if surgical complication rate <3% (reduces 5-year ipsilateral stroke risk in men) |
| Venous sinus thrombosis | Heparin/LMWH → warfarin; DOACs under investigation |
5. Rehabilitation
Physical, occupational, and speech therapy are critical components with clear evidence of benefit on post-stroke functional outcomes. Swallowing assessment before oral feeding is mandatory in patients with dysphagia, dysarthria, or facial droop. (Washington Manual of Medical Therapeutics)
Recent Evidence Updates
- Tenecteplase vs. Alteplase (PMID 39413337): 2024 systematic review confirms non-inferiority within 4.5 hours — guidelines increasingly recommend tenecteplase as a practical alternative
- Late-window thrombolysis (PMID 39882605): 2025 meta-analysis supports tPA beyond 4.5 hours in imaging-selected patients
- Basilar artery thrombectomy (PMID 39512275): 2024 systematic review supports thrombectomy ± thrombolysis for basilar artery occlusion
Sources: Rosen's Emergency Medicine (9e) | Bradley & Daroff's Neurology in Clinical Practice | Washington Manual of Medical Therapeutics | AHA/ASA 2019 Acute Ischemic Stroke Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.