Pfn
Asking for Preferences
Asking for Preferences
Reading File
Searching the Web
Proximal Femoral Nail design components overview
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material to write a thorough overview. Here is the full answer:
Proximal Femoral Nail (PFN) - Overview & Design
What Is It?
The PFN is an intramedullary (IM) implant - more precisely, a type of cephalomedullary nail - used to fix fractures of the proximal femur, particularly intertrochanteric and subtrochanteric fractures. The nail sits inside the femoral medullary canal and is anchored proximally into the femoral head/neck, giving it a mechanical advantage over extramedullary devices like the sliding hip screw (DHS/CHS).
Core Components
| Component | Description |
|---|---|
| Main nail (intramedullary rod) | Titanium or stainless steel cannulated rod inserted into the femoral canal; proximal diameter ~17 mm, distal ~10 mm |
| Femoral neck screw (lag screw) | Large sliding screw (11 mm diameter, lengths 80-120 mm) that passes through the nail into the femoral head; CCD angles of 125° or 130° |
| Anti-rotation / hip pin | A secondary 6.5 mm self-tapping pin placed parallel and superior to the lag screw to prevent rotation of the femoral head fragment |
| Distal locking bolts | One or two 4.9 mm screws placed transversely through the nail at the distal end; can be placed statically (rigid, length-stable) or dynamically (allows axial compression) |
| End cap | Plugs the distal tip of the nail; prevents bone ingrowth and aids future removal |
Key Design Features
- Anatomical nail geometry: 6° mediolateral (ML) angle allowing entry at or just lateral to the tip of the greater trochanter (piriformis entry or trochanteric entry, depending on version); also has a ~10° anteversion built into the proximal portion
- Antecurvature (1.5 m radius): Matches the natural anterior bow of the femur to reduce stress concentration and ease insertion
- Cannulated throughout: Allows guide-wire-assisted insertion under fluoroscopic control
- Flexible distal tip: Reduces stress-riser effect at the nail tip, lowering the risk of peri-implant fracture
- Two proximal screws (lag + anti-rotation pin): This is the hallmark feature distinguishing classic PFN from a Gamma nail (which uses only one lag screw). The dual-screw design provides rotational control of the femoral head fragment
Short vs. Long PFN
| Short PFN | Long PFN | |
|---|---|---|
| Length | ~200-240 mm (3 sizes: 340/380/420 mm for standard) | Up to femoral condyles |
| Use | Intertrochanteric fractures not extending >3 cm below trochanteric region | Subtrochanteric fractures, fractures with long distal extension, pathologic fractures |
| Locking | May leave unlocked in stable patterns | Distal locking mandatory |
For most trochanteric fractures, current evidence recommends a short cephalomedullary nail - results are equivalent to long nails for fractures not extending below 3 cm of the trochanteric region.
Biomechanical Rationale
The IM position of the nail places it much closer to the mechanical axis of the femur compared to a lateral plate, resulting in:
- Shorter bending moment arm
- Better load sharing
- Less risk of implant failure under cyclic loading
- Reduced femoral medialization and shaft collapse compared to the sliding hip screw in unstable (AO/OTA 31-A2 and A3) patterns
The dual-screw configuration (lag screw + anti-rotation pin) creates a more stable fixation of the femoral head fragment, preventing rotation (the "egg-cup" effect seen with single-screw systems in osteoporotic bone).
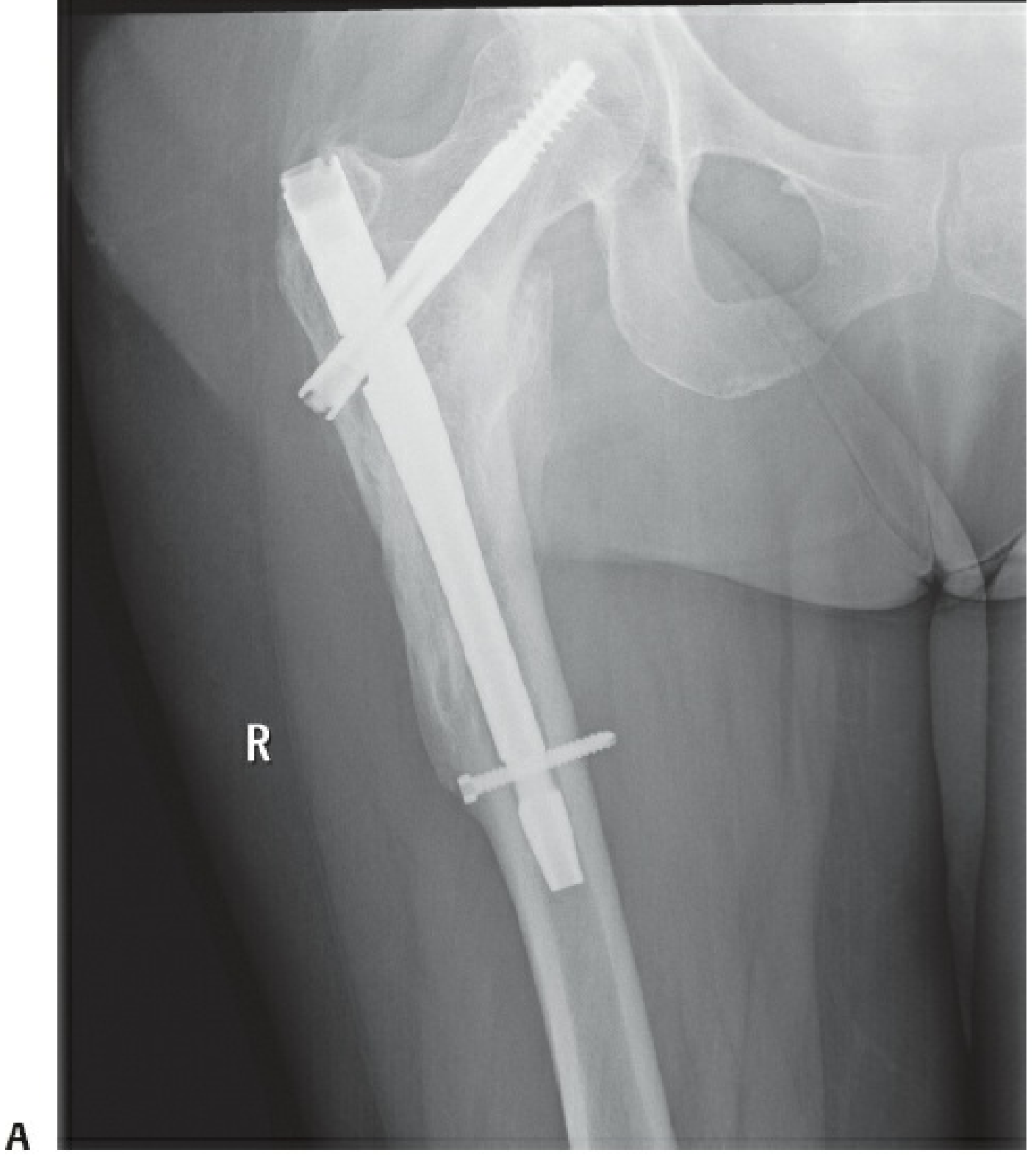
AP radiograph of a cephalomedullary nail (PFN type) in the right proximal femur, showing the intramedullary rod, the lag screw in the femoral head, and distal locking bolts - Rockwood and Green's Fractures in Adults, 10th ed. 2025
PFN vs. Related Implants
| Implant | Proximal fixation | Key difference |
|---|---|---|
| Classic PFN (AO/Synthes) | Lag screw + anti-rotation pin (2 screws) | Original design; dual screw construct |
| PFNA (PFN Antirotation) | Single helical blade | Blade compacts bone rather than removing it; better in osteoporotic bone; 1 proximal element |
| Gamma Nail | Single large lag screw | First widely used IM nail for this indication; higher complication rate with early designs |
| InterTAN | Two integrated cephalomedullary screws with linear compression | Interlocking proximal screws resist rotation; may offer lower cutout rate |
| DHS (sliding hip screw) | Single lag screw + lateral plate | Extramedullary; still acceptable for stable A1 fractures |
Clinical Status
Current guidelines (supported by large registry data) favour cephalomedullary nails (including PFN and its derivatives) over the sliding hip screw for unstable intertrochanteric fractures (AO/OTA 31-A2, A3) because they reduce reoperation rates and may slightly lower mortality. For stable A1 fractures, both the sliding hip screw and short IM nail remain acceptable options.
- Rockwood and Green's Fractures in Adults, 10th ed. 2025 - Cephalomedullary Implants section
- Campbell's Operative Orthopaedics, 15th ed. 2026 - Intertrochanteric Fractures chapter
- AO Foundation PFNA overview
This is a shared conversation. Sign in to Orris to start your own chat.