Small bowel intestinal bacterial overgrowth internal medicine Pathogenesis Diagnosis Symptoms Treatment Lab investigations Complications Patient presented with the same with clinical case
Reading File
Finding Sources
Finding Sources
Searching PubMed
"small intestinal bacterial overgrowth" AND diagnosis AND treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Searching Images
small intestinal bacterial overgrowth SIBO pathogenesis diagram
Finding Sources
Loading Image
Finding Sources
Reading File
I have all the content needed. Let me now compile the comprehensive SIBO response:
Small Intestinal Bacterial Overgrowth (SIBO)
Internal Medicine – Comprehensive Review
Normal Intestinal Flora Baseline
The small intestine normally maintains a very low bacterial load (~10³ CFU/mL), in contrast to the colon (up to 10¹² CFU/mL). This is maintained by several protective mechanisms:
- Bactericidal gastric acid and bile
- Normal intestinal motility (mean small bowel transit ~84 min)
- Mucosal immunological defenses (secretory IgA)
- Ileocecal valve integrity preventing retrograde colonic colonization
Bacterial titers increase progressively from the duodenum to the ileum. SIBO is defined as abnormal colonization of the small intestine, typically with coliform or mixed flora, in concentrations >10⁵ CFU/mL on jejunal aspirate culture.
Pathogenesis
Predisposing Conditions (by mechanism)
1. Decreased Motility / Stasis
- Scleroderma (pseudo-obstruction from smooth muscle fibrosis)
- Chronic intestinal pseudo-obstruction
- Diabetes mellitus (autonomic neuropathy → gastroparesis / dysmotility)
- Irritable bowel syndrome
- Celiac disease
- Cirrhosis with portal hypertension
- Chronic renal disease
- Elderly patients (reduced motility, hypochlorhydria)
2. Anatomic Causes / Blind Loops
- Roux-en-Y gastric bypass (afferent limb)
- Billroth II anastomosis
- Small bowel diverticulosis (jejunal diverticula)
- Strictures: Crohn's disease, radiation, NSAIDs, surgical adhesions
- Malignant tumors: carcinoid, adenocarcinoma, lymphoma
- Benign tumors: adenomas, lipomas, leiomyoma
3. Altered Bacterial Load Mechanisms
- Surgical resection of the ileocecal valve (allows colonic backwash)
- Gastrojejunostomy / enteroenteric fistulae (Crohn's disease)
- Hypochlorhydria: chronic PPI use (reduces acid-mediated bactericidal activity)
- Immune deficiency: IgA deficiency, HIV/AIDS, common variable immunodeficiency
- Acute pancreatitis
Metabolic Consequences of Overgrowth
| Mechanism | Consequence |
|---|---|
| Bacterial deconjugation of bile acids → absorbed in proximal bowel | Intraluminal bile acid deficiency → fat malabsorption, steatorrhea |
| Brush border damage → carbohydrate maldigestion | Short-chain fatty acid production → osmotic diarrhea, gas, bloating |
| Bacterial consumption of vitamin B₁₂ | Macrocytic (megaloblastic) anemia, peripheral neuropathy |
| Bacterial synthesis of folate | Elevated serum folate (paradoxically normal/high) |
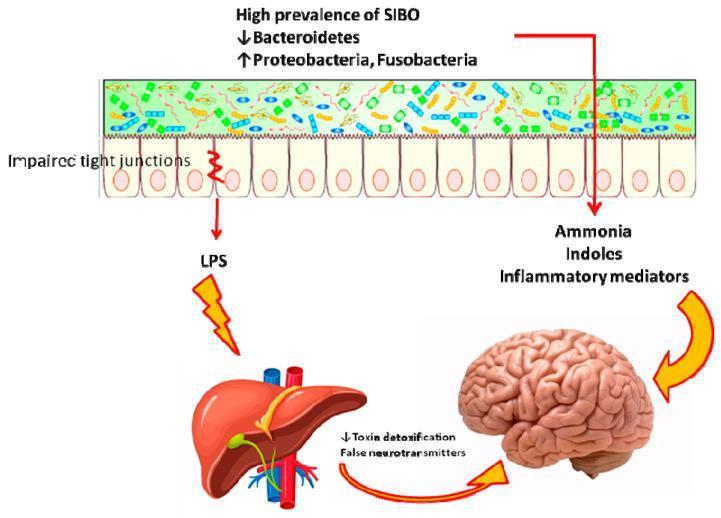
| Increased intestinal permeability ("leaky gut") | Translocation of LPS → systemic endotoxemia |
| Enterocyte damage, villous blunting | Malabsorption of fat-soluble vitamins (A, D, E, K) |
Clinical Symptoms
| Symptom | Mechanism |
|---|---|
| Bloating / flatulence | Bacterial fermentation of carbohydrates → gas production |
| Abdominal pain / cramping | Luminal distension, increased intraluminal pressure |
| Chronic watery diarrhea | Carbohydrate maldigestion + short-chain fatty acid production |
| Steatorrhea | Bile acid deconjugation → fat malabsorption |
| Weight loss / malnutrition | Global malabsorption |
| Fatigue, pallor | B₁₂-deficiency macrocytic anemia |
| Peripheral neuropathy | B₁₂ deficiency (subacute combined degeneration) |
| Night blindness / osteoporosis | Fat-soluble vitamin deficiencies (A, D, K) |
| Edema / hypoproteinemia | Protein-losing enteropathy from mucosal damage |
Note: Symptoms overlap substantially with IBS (bloating, pain, altered bowel habit), and SIBO has been demonstrated in patients with diarrhea-predominant IBS; treatment of overgrowth leads to symptom resolution in a subset. — Harrison's Principles of Internal Medicine, 22e (2025)
Laboratory Investigations
| Test | Finding in SIBO |
|---|---|
| CBC | Macrocytic anemia (↑ MCV), normochromic |
| Serum Vitamin B₁₂ | ↓ Low (bacterial consumption) |
| Serum Folate | ↑ Elevated (bacterial synthesis) |
| Serum albumin / pre-albumin | ↓ Low (malnutrition, protein-losing enteropathy) |
| Fat-soluble vitamins (A, D, E, K) | ↓ Low |
| Prothrombin time | ↑ Prolonged (vitamin K deficiency) |
| Stool fat (72-hour) | ↑ Elevated (steatorrhea) |
| Fecal elastase | Normal (distinguishes from exocrine pancreatic insufficiency) |
| CRP / ESR | May be mildly elevated |
| Peripheral smear | Macrocytes, hypersegmented neutrophils |
Diagnosis
Gold Standard
Quantitative culture of small-intestinal (jejunal) aspirate: ≥10⁵ CFU/mL of non-indigenous bacteria, or ≥10³ CFU/mL with coliform flora. Obtained via upper endoscopy with aspiration. Technically demanding and not widely available in routine practice.
- Additional testing on aspirate: measurement of deconjugated bile acids, vitamin B₁₂ analogs.
Breath Hydrogen Testing (Widely Available)
Bacteria ferment carbohydrate substrates → H₂ and/or CH₄ absorbed and exhaled.
| Test | Substrate | Interpretation |
|---|---|---|
| Glucose H₂ breath test | 75g glucose | Rise >12–20 ppm over baseline at <90 min = positive (high specificity) |
| Lactulose H₂ breath test | 10g lactulose (nondigestible) | Early peak in H₂ before cecal peak; prone to false positives |
| ¹⁴C-glycocholate breath test | Labeled bile acid | Measures bile acid deconjugation |
| ¹⁴C-d-xylose breath test | Labeled xylose | Bacterial metabolism → ¹⁴CO₂ exhaled |
Cautions with breath testing:
- False positives from: rapid transit (early cecal fermentation), oral flora, prior antibiotics
- False negatives: slow transit, prior antibiotics, methane producers (require CH₄ measurement)
- Must fast overnight; no antibiotics for 4 weeks prior; no high-fiber diet
Empirical Treatment Trial
Many clinicians empirically treat with antibiotics and observe for symptom resolution — this is widely accepted in clinical practice given the limitations of breath testing. — Harrison's 22e, Yamada's Gastroenterology 7e
Imaging (Indirect)
- Barium contrast small bowel follow-through / CT enterography: may reveal underlying causes (diverticula, strictures, blind loops, fistulae — see figure below)
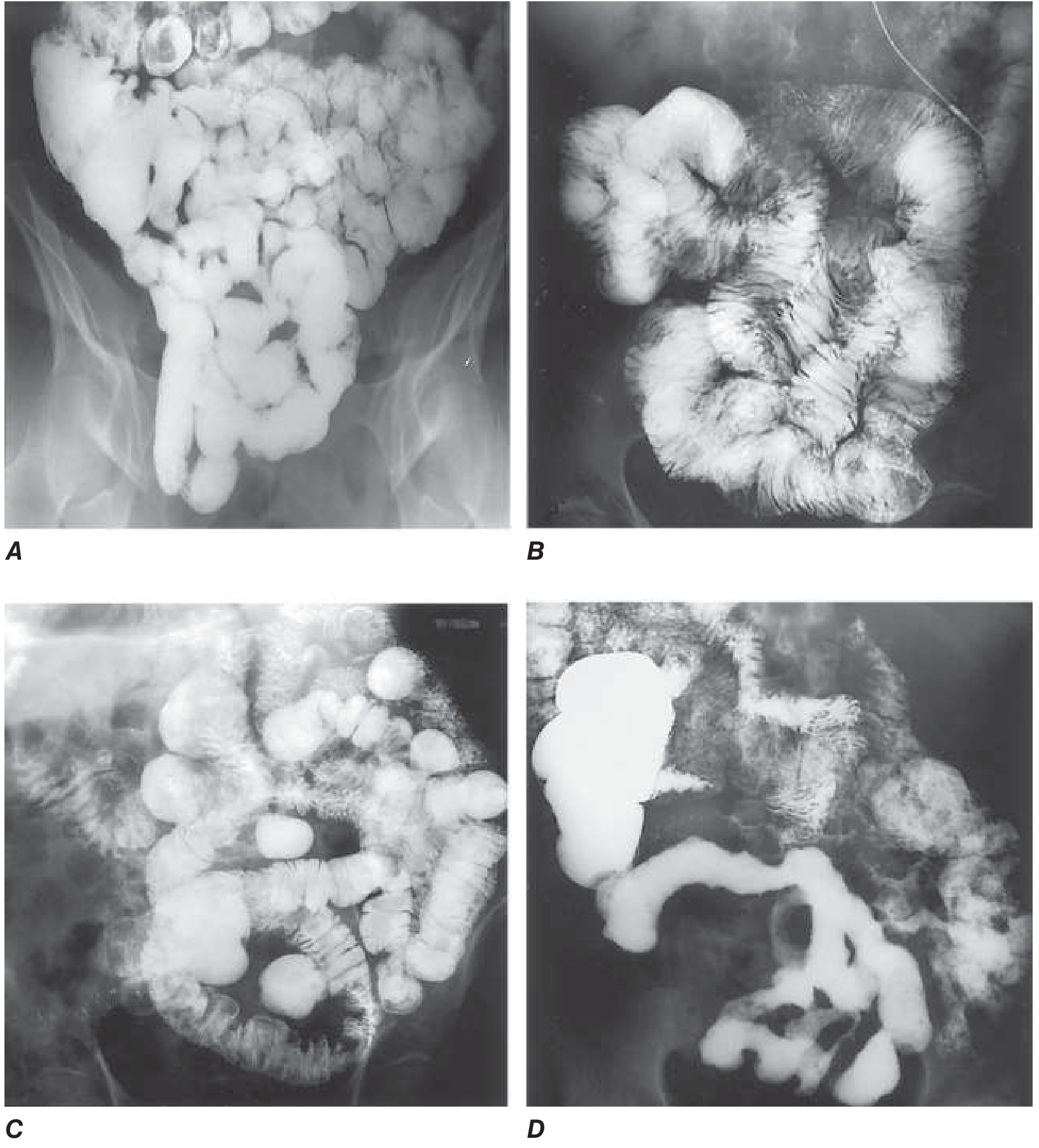
(A) Normal small bowel; (B) Celiac disease; (C) Jejunal diverticulosis — a SIBO predisposing condition; (D) Crohn's disease with strictures — Harrison's Fig. 336-3
Treatment
1. Treat Underlying Cause (Definitive)
- Surgical correction of blind loops, resection of large diverticula
- Endoscopic/surgical treatment of strictures
- Treat Crohn's disease to prevent recurrent fibrosis
- Stop/reduce PPIs if clinically feasible
2. Antibiotic Therapy (First-Line)
Rifaximin is the most studied and preferred agent:
- Non-absorbable antibiotic — minimal systemic absorption, low resistance
- Dose: 550 mg TID × 14 days (or 1200 mg/day × 14 days)
- Efficacy (symptom improvement or breath test normalization): 34–87.5%
- Evidence from meta-analyses supports use in both SIBO and SIBO-associated IBS
Other antibiotics used:
| Antibiotic | Notes |
|---|---|
| Metronidazole 250–500 mg TID × 7–10 days | Good anaerobic coverage |
| Doxycycline 100 mg BD × 7–10 days | Broad spectrum |
| Amoxicillin-clavulanate 875/125 mg BD × 7–10 days | Covers aerobes + anaerobes |
| Cephalosporins (e.g., cephalexin) | Alternative option |
| Norfloxacin / ciprofloxacin | Used in some regimens |
Rotating antibiotics: For recurrent/chronic SIBO (especially in dysmotility disorders like scleroderma), cyclical antibiotic courses (1–2 weeks per month with alternating agents) are used.
Due to increasing antibiotic resistance, empiric treatment without diagnostic confirmation is not universally recommended, particularly when alternative diagnoses are plausible. — Yamada's Gastroenterology 7e
3. Nutritional Support
- Vitamin B₁₂ supplementation (IM if severe deficiency)
- Fat-soluble vitamins (A, D, E, K) replacement
- Nutritional support for severe malnutrition (enteral ± parenteral)
- Dietary modification: reduce fermentable carbohydrates (low-FODMAP diet may help symptoms)
4. Probiotics
A 2024 systematic review and meta-analysis (PMID: 39538392) found probiotics have some efficacy in SIBO treatment; however, evidence remains mixed. Probiotics are considered adjunctive rather than primary therapy.
5. Prokinetics (for Dysmotility)
- Metoclopramide, domperidone, erythromycin (low-dose), prucalopride — improve intestinal transit and reduce bacterial stasis
- Particularly relevant in scleroderma and diabetic enteropathy
Complications
| Complication | Mechanism |
|---|---|
| Megaloblastic anemia | Vitamin B₁₂ depletion by bacteria |
| Peripheral neuropathy | B₁₂ deficiency (subacute combined degeneration of spinal cord) |
| Osteomalacia / osteoporosis | Vitamin D and calcium malabsorption |
| Night blindness / xerophthalmia | Vitamin A deficiency |
| Bleeding diathesis / coagulopathy | Vitamin K deficiency |
| Protein-losing enteropathy | Mucosal damage → hypoalbuminemia, edema |
| Malnutrition / cachexia | Global malabsorption + weight loss |
| Hepatic encephalopathy (in cirrhosis) | LPS translocation → ↑ systemic endotoxemia + ammonia production |
| Dehydration / electrolyte imbalance | Chronic diarrhea |
Clinical Case
Presentation
Patient: 58-year-old male with a background of long-standing type 2 diabetes mellitus (15 years, poorly controlled HbA1c 9.2%) and chronic PPI use (omeprazole 40 mg OD for 5 years for GERD).
Chief Complaint: 6-month history of chronic, non-bloody, foul-smelling diarrhea (4–6 loose stools/day), progressive abdominal bloating, flatulence, and 8 kg weight loss.
History: Reports floating, greasy stools worsening over months. Intermittent crampy peri-umbilical pain. No fever, no blood/mucus in stool. No recent travel, no alcohol use.
Medications: Metformin, insulin glargine, omeprazole.
Physical Examination:
- BMI 20.2 (down from 24.0)
- Pallor +++, mild glossitis
- Abdomen: distended, mild diffuse tenderness, hyperactive bowel sounds
- No lymphadenopathy, no hepatosplenomegaly
- Neurological: reduced vibration sense bilateral lower limbs, normal power
Investigations
| Test | Result | Interpretation |
|---|---|---|
| Hb | 8.4 g/dL | Anemia |
| MCV | 108 fL | Macrocytosis |
| Peripheral smear | Macrocytes, hypersegmented neutrophils | Megaloblastic anemia |
| Serum B₁₂ | 98 pg/mL (↓) | Deficient (ref 200–900) |
| Serum folate | 28 ng/mL (↑) | Elevated — bacterial synthesis |
| Serum albumin | 2.8 g/dL (↓) | Hypoalbuminemia |
| 72-hr stool fat | Elevated | Steatorrhea |
| Vitamin D | 14 ng/mL (↓) | Deficient |
| Prothrombin time | 17s (↑) | Vitamin K deficiency |
| Fasting glucose | 14 mmol/L | Poor diabetic control |
| Fecal elastase | Normal | EPI excluded |
| Glucose H₂ breath test | H₂ rise >20 ppm at 60 min | Positive for SIBO |
| CT abdomen | Small bowel dilatation; no structural obstruction | Consistent with dysmotility |
Diagnosis
Small Intestinal Bacterial Overgrowth (SIBO) secondary to:
- Diabetic autonomic neuropathy → intestinal dysmotility/stasis
- Chronic PPI use → hypochlorhydria → impaired acid defense
Management
- Rifaximin 550 mg TID × 14 days (first-line non-absorbable antibiotic)
- Vitamin B₁₂ intramuscular injection 1000 mcg daily × 7 days, then monthly
- Vitamin D supplementation 50,000 IU weekly × 8 weeks
- Vitamin K oral supplementation
- Review and dose-reduce/stop omeprazole if clinically feasible (address the contributing factor)
- Optimize glycemic control — tighten HbA1c to reduce autonomic neuropathy progression; consider addition of a prokinetic
- Low-FODMAP diet counseling to reduce fermentable substrate
- Prokinetic therapy (e.g., low-dose erythromycin or prucalopride) to improve motility
- Nutritional support — high-protein diet, monitor nutritional markers
- Repeat glucose H₂ breath test at 4 weeks to confirm eradication; re-treat if symptoms recur
Outcome expectation: Symptom improvement (bloating, diarrhea) typically within 1–2 weeks of antibiotic initiation. Anemia corrects over weeks with B₁₂ replacement. Given ongoing dysmotility, this patient is at high risk for recurrence and may require cyclical antibiotic prophylaxis.
Summary Table
| Domain | Key Points |
|---|---|
| Normal flora | Small bowel <10³ CFU/mL; colon up to 10¹² CFU/mL |
| SIBO threshold | >10⁵ CFU/mL on jejunal aspirate |
| Key mechanisms | Dysmotility, anatomic stasis, hypochlorhydria, ileocecal valve loss, immune deficiency |
| Classic presentation | Bloating, diarrhea, steatorrhea, B₁₂ deficiency, elevated folate |
| Gold standard diagnosis | Jejunal aspirate culture >10⁵ CFU/mL |
| Practical diagnosis | Glucose hydrogen breath test (more specific than lactulose) |
| First-line treatment | Rifaximin 550 mg TID × 14 days |
| Key complications | Megaloblastic anemia, neuropathy, osteomalacia, hypoalbuminemia |
| Recurrence | Common in dysmotility syndromes; cyclical antibiotics needed |
Sources: Harrison's Principles of Internal Medicine, 22nd ed. (2025); Yamada's Textbook of Gastroenterology, 7th ed.; Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Niño et al. (2024) Syst. Review [PMID 39538392]; Lu H. (2026) SIBO–IBS meta-analysis [PMID 41883799]
This is a shared conversation. Sign in to Orris to start your own chat.