Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I have sufficient information from the textbooks. Now let me compose a comprehensive answer.
Case Analysis: 55-Year-Old Male with Acute Chest Pain
a) Diagnosis
ST-Elevation Myocardial Infarction (STEMI)
The clinical picture is classic:
- Acute-onset chest pain in a middle-aged male
- Radiation to the left shoulder and arm (referred pain via C8-T4 dermatomes)
- ECG showing ST-segment elevation and T-wave inversion
ST elevation indicates full-thickness (transmural) myocardial ischemia/injury, while T-wave inversion reflects evolving ischemia. Together, they meet the diagnostic criteria for STEMI, which requires emergency reperfusion therapy (primary PCI or thrombolysis).
b) Etiopathogenesis
The underlying mechanism in the vast majority (~90%) of STEMI cases is acute coronary thrombosis superimposed on atherosclerotic plaque disruption. The sequence is:
-
Atherosclerotic plaque formation - Years of lipid deposition, foam cell accumulation, and chronic inflammation create an atheromatous plaque within a coronary artery. Importantly, the culprit plaque often does NOT cause a critical stenosis (>70%) beforehand.
-
Plaque disruption - Endothelial injury, mechanical forces, or intraplaque hemorrhage causes sudden erosion or rupture of the fibrous cap, exposing subendothelial collagen and necrotic plaque contents to circulating blood.
-
Platelet activation and aggregation - Exposed collagen triggers platelet adhesion. Activated platelets release thromboxane A2, ADP, and serotonin, which amplify further platelet aggregation and induce vasospasm.
-
Coagulation cascade activation - Exposed tissue factor activates the extrinsic coagulation pathway, generating thrombin and adding to the growing thrombus.
-
Complete luminal occlusion - Within minutes, the enlarging thrombus totally occludes the coronary artery, cutting off blood supply to the downstream myocardium.
-
Myocardial ischemia and necrosis - Loss of aerobic metabolism occurs within seconds. ATP falls and toxic metabolites (lactate) accumulate. Contractility is lost within 1-2 minutes. If ischemia persists beyond 20-40 minutes, irreversible coagulative necrosis of myocytes ensues. Necrosis begins in the subendocardial zone (most vulnerable, furthest from epicardial vessels and under highest intramural pressure) and progresses as a "wavefront" toward the epicardium.
(Sources: Robbins & Kumar Basic Pathology, p. 354; Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 511)
Less common causes (~10%) include coronary vasospasm (e.g., cocaine use), emboli (from mural thrombi in AF, valve vegetations), vasculitis, or hematologic disorders (e.g., sickle cell disease).
c) Immediate Complications
| Complication | Mechanism / Notes |
|---|---|
| Arrhythmias | Most common early complication. Ischemic myocytes become electrically unstable (irritable), forming reentry circuits that can lead to ventricular tachycardia and ventricular fibrillation (VF). VF is the leading cause of death in ~80-90% of cardiac deaths in acute MI. |
| Cardiogenic shock / Acute LV failure | Large infarcts (>40% of LV mass) impair pump function severely, causing acute heart failure and cardiogenic shock. |
| Ventricular free wall rupture | Occurs within the first 3-5 days as necrotic myocardium softens. Leads to hemopericardium and tamponade - frequently fatal. |
| Ventricular septal defect (VSD) | Rupture of the interventricular septum creates an acute left-to-right shunt, causing acute right heart failure. |
| Papillary muscle rupture / dysfunction | Ischemia or rupture of the papillary muscles causes acute mitral regurgitation with sudden onset pulmonary edema. |
| Pericarditis (Fibrinous) | Transmural infarction causes overlying pericardial inflammation within 1-3 days (Dressler's syndrome occurs later at 2-10 weeks). |
| Mural thrombus | Damaged endocardium and akinetic wall segment promote thrombus formation, risking systemic embolization (stroke, limb ischemia). |
| Right ventricular infarction | Particularly with inferior STEMI (RCA occlusion), causing hypotension without pulmonary congestion. |
(Sources: Robbins & Kumar Basic Pathology, p. 380; Robbins, Cotran & Kumar Pathologic Basis of Disease)
The most immediately life-threatening complications are ventricular fibrillation and cardiogenic shock, which is why rapid ECG recognition and emergency reperfusion are the cornerstone of STEMI management.
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information. Let me compose the full answer.
Case Analysis: 60-Year-Old Chronic Alcoholic with Hematemesis, Drowsiness, Icterus, and Ascites
a) Diagnosis
Alcoholic Liver Cirrhosis with Portal Hypertension
The constellation of findings points directly to end-stage alcohol-related liver disease:
| Finding | Explanation |
|---|---|
| Chronic alcoholic | Primary etiology - 15-20 years of excess intake leads to cirrhosis |
| Hematemesis | Bleeding from esophageal varices secondary to portal hypertension |
| Drowsy / disoriented | Hepatic encephalopathy - failure of ammonia detoxification |
| Icterus (jaundice) | Impaired bilirubin conjugation and excretion by failing hepatocytes |
| Ascites | Portal hypertension + hypoalbuminemia (reduced hepatic synthesis) |
The organ involved is the liver.
b) Gross and Microscopic Morphology of the Liver
Alcohol-related liver disease passes through three overlapping morphologic stages: steatosis → steatohepatitis → fibrosis/cirrhosis.
Gross Morphology
Early (steatosis/steatohepatitis stage):
- Liver is large, soft, yellow, and greasy - may weigh 4-6 kg or more
- Yellow-tan discoloration from accumulated fat
- Surface is smooth at this stage
End-stage (cirrhosis):
- Liver is small, brown, and shrunken
- Surface is covered by diffuse micronodules (nodules typically < 0.3 cm in diameter - smaller than in viral hepatitis-related cirrhosis - hence micronodular cirrhosis)
- Fibrous bands are visible separating the nodules
- The "burned-out" cirrhotic liver may lose its fatty appearance
Here is the gross appearance of a cirrhotic liver:

Microscopic Morphology
1. Hepatocellular Steatosis (Fatty change):
- Small (microvesicular) and large (macrovesicular) lipid droplets within hepatocytes
- Begins in centrilobular hepatocytes (zone 3), spreads outward
- Large droplets displace the nucleus to the periphery of the cell
- Characteristic perisinusoidal fibrosis in a "chicken-wire fence" pattern
2. Steatohepatitis changes:
- Hepatocyte ballooning - cell swelling and necrosis, most pronounced in centrilobular regions
- Mallory hyaline bodies (Mallory-Denk bodies) - tangled skeins of ubiquitinylated keratins 8 and 18, seen as eosinophilic cytoplasmic inclusions in degenerating hepatocytes - a hallmark of alcoholic hepatitis
- Neutrophilic infiltration - neutrophils permeate the lobule and accumulate around hepatocytes containing Mallory bodies; lymphocytes and macrophages in portal tracts
3. Fibrosis and Cirrhosis:
- Begins as central vein sclerosis and perisinusoidal fibrosis
- Fibrous bands link central veins to portal tracts (central-portal bridging fibrosis)
- Progressive subdivision of parenchyma into micronodules surrounded by fibrous septa
- Complete architectural distortion of the normal lobular pattern
- Ductular reactions (duct-like structures from stem cell activation) increase with progression
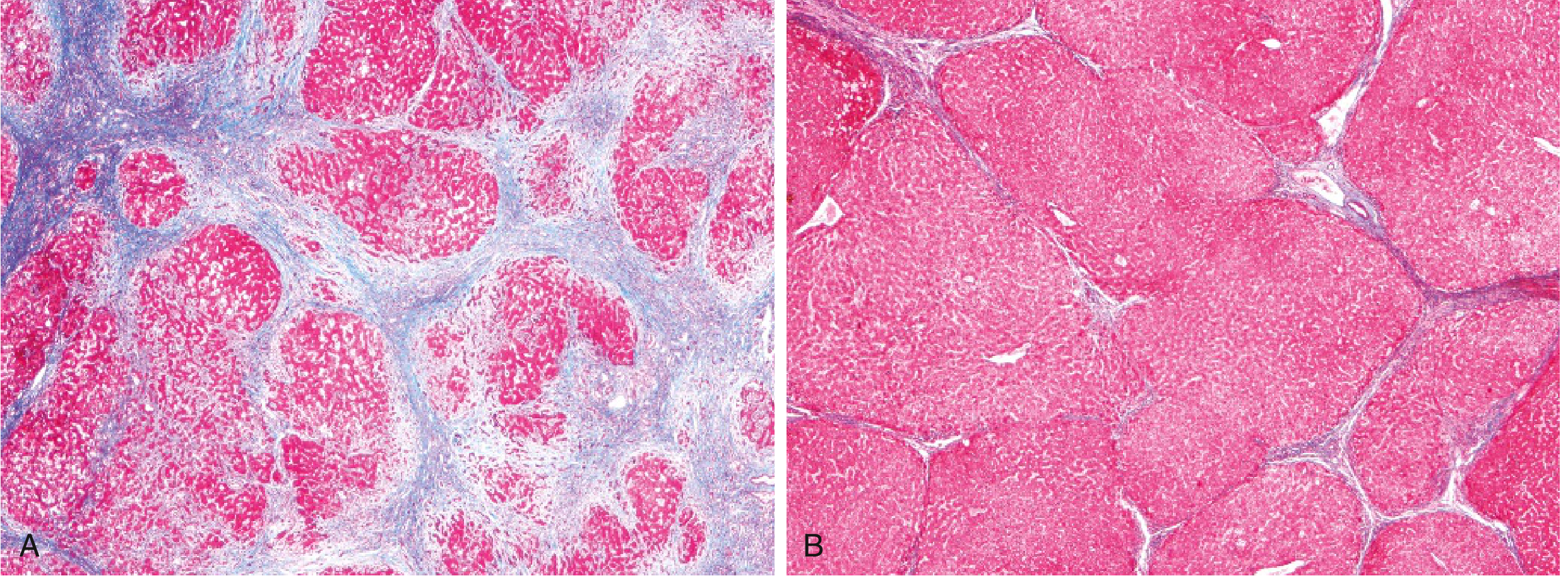
(Source: Robbins & Kumar Basic Pathology)
c) Complications of Alcoholic Liver Cirrhosis
From Portal Hypertension:
- Esophageal/gastric varices - dilated portosystemic collateral veins that can rupture, causing massive hematemesis (the presenting symptom here). Occur in ~40% of advanced cirrhosis cases.
- Ascites - transudative fluid accumulation in the peritoneal cavity (serum-to-ascites albumin gradient ≥1.1 g/dL). About 85% of all ascites cases are due to cirrhosis.
- Congestive splenomegaly - splenic weight may reach up to 1000 g (5-6x normal), leading to hypersplenism with thrombocytopenia and pancytopenia.
- Caput medusae - dilated periumbilical veins from recanalized umbilical vein.
From Hepatocellular Failure:
- Hepatic encephalopathy - failure to detoxify ammonia and other gut-derived toxins; presents as confusion, drowsiness, and disorientation (as in this patient).
- Jaundice / coagulopathy - impaired bilirubin conjugation and reduced synthesis of clotting factors (II, VII, IX, X).
- Hypoalbuminemia - reduced synthetic function contributing to peripheral edema and ascites.
- Hyperestrogenemia (in males) - impaired estrogen metabolism causes palmar erythema, spider angiomas, gynecomastia, and hypogonadism.
Infective and Renal Complications:
- Spontaneous bacterial peritonitis (SBP) - infection of ascitic fluid; increased susceptibility due to impaired immune function.
- Hepatorenal syndrome - functional renal failure from splanchnic vasodilation and reduced effective renal perfusion; a pre-terminal event.
Neoplastic Complication:
- Hepatocellular carcinoma (HCC) - develops in 10-20% of patients with alcohol-related cirrhosis.
Terminal causes of death:
- Hepatic failure
- Massive GI hemorrhage (variceal bleed)
- Intercurrent infection
- Hepatorenal syndrome
- Hepatocellular carcinoma (3-6% of cases)
(Sources: Robbins & Kumar Basic Pathology, pp. 598-611; Robbins, Cotran & Kumar Pathologic Basis of Disease)
This is a shared conversation. Sign in to Orris to start your own chat.