Case on neurocyticersis
Reading File
Finding Sources
Finding Sources
Searching PubMed
neurocysticercosis diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
neurocysticercosis MRI CT brain cyst scolex
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information to compile a detailed clinical case on neurocysticercosis. Let me present it:
Neurocysticercosis (NCC) — Clinical Case & Review
Case Presentation
Patient: 34-year-old male, originally from Mexico, residing in the United States for 8 years.
Chief Complaint: New-onset generalized tonic-clonic seizure.
History: No prior seizure history. Reports intermittent headaches over the past 3 months. No fever. No known prior epilepsy. Family members in Mexico raise pigs.
Examination: Post-ictal confusion resolving over 30 minutes. Neurological exam otherwise normal. No papilledema on fundoscopy initially.
Background & Epidemiology
Neurocysticercosis is the most common parasitic disease of the CNS worldwide and the most common cause of symptomatic epilepsy globally. It is caused by the larval stage of Taenia solium, the pork tapeworm. — Bradley and Daroff's Neurology in Clinical Practice, p. 980
Estimated burden:
- 0.45–1.35 million with NCC-related epilepsy in Latin America
- ~1 million in India
- 0.31–4.6 million in Africa
- 1,320–5,050 new cases per year in the United States, driven by immigration from endemic regions
Developing countries with poor sanitation, open defecation near pig farms, and consumption of undercooked pork are the primary endemic regions. — Bradley and Daroff's Neurology in Clinical Practice, p. 980
Pathogenesis & Life Cycle
Humans can become both the definitive host (intestinal tapeworm, via eating undercooked pork) and the intermediate host (larval cysts in tissues, via fecal-oral transmission of eggs).
- Taeniasis (intestinal): Human ingests undercooked pork containing cysticerci → adult tapeworm in intestine → proglottids shed eggs in stool
- Cysticercosis (larval): Human ingests T. solium eggs (from contaminated food, water, autoinfection, or a tapeworm carrier in the household) → eggs hatch in intestine, releasing oncospheres → penetrate gut wall → disseminate hematogenously to CNS, muscle, eye, subcutaneous tissue
- Once in CNS, larvae mature into cysticercus: a fluid-filled bladder containing an invaginated scolex
Key Point: A person does not need to eat pork to develop NCC — ingestion of T. solium eggs (fecal-oral route from a tapeworm carrier) is sufficient. — Sherris & Ryan's Medical Microbiology, p. 1541; Goldman-Cecil Medicine
Classification
| Type | Location | Clinical Features |
|---|---|---|
| Parenchymal NCC | Brain tissue | Seizures, focal deficits |
| Intraventricular NCC | Ventricles | Obstructive hydrocephalus, Bruns syndrome |
| Subarachnoid NCC | Basal cisterns/convexity | Meningitis, vasculitis, hydrocephalus |
| Spinal NCC | Spinal cord/roots | Myelopathy, radiculopathy (mimics tumor) |
| Ocular NCC | Vitreous, retina | Visual disturbance, floaters |
Stages of the Disease (Pathological & Radiological)
There are four recognized stages: — Harrison's Principles of Internal Medicine 22E, p. 1181
| Stage | Parasite Status | MRI/CT Appearance | Edema | Treatment |
|---|---|---|---|---|
| Vesicular | Viable larva (live scolex visible) | Cyst with a dot (scolex) — "hole-with-dot" sign; no enhancement | None | Anticysticidal therapy |
| Colloidal vesicular | Degenerating larva | Ring enhancement on contrast; surrounding edema on T2/FLAIR | Present (significant) | Anticysticidal + steroids |
| Granulonodular | Dead larva, granuloma forming | Homogeneous nodular enhancement; reducing edema | Minimal | Controversial (some treat) |
| Nodular calcified | Dead, calcified | Hyperdense nodule on CT; difficult to see on MRI; use SWI | None | No anticysticidal therapy |
Most sensitive MRI sequence for small calcifications: Susceptibility-Weighted Imaging (SWI). — Harrison's, p. 1181
Neuroimaging
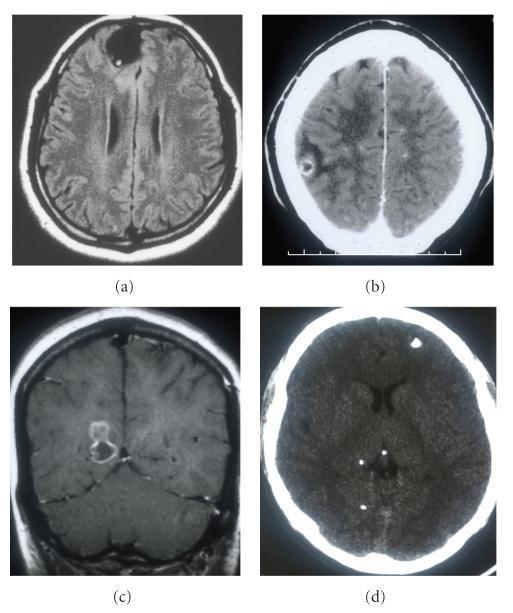
Above: Four radiological stages of parenchymal NCC. (a) Vesicular stage — FLAIR shows "hole-with-dot" cyst, no edema. (b) Colloidal stage — CT shows degenerating cyst with perilesional edema and ring enhancement. (c) Granular-nodular stage — enhancing thickened wall. (d) Calcified stage — CT shows hyperdense calcified nodules.
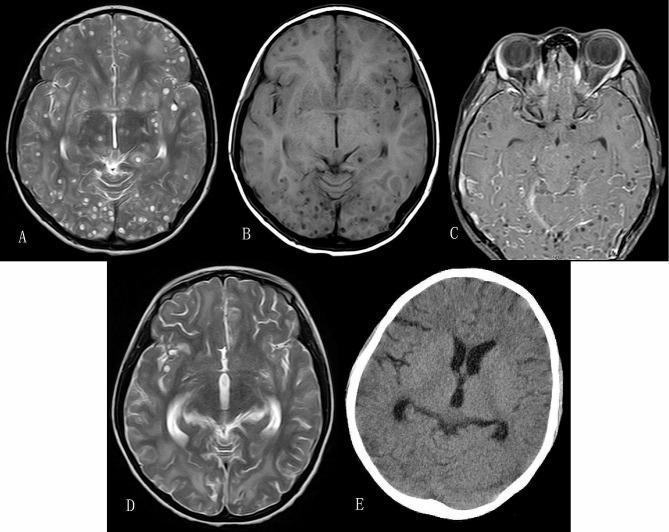
Above: Heavy NCC burden on T2/T1 MRI (panels A–D) showing multiple vesicular cysts with the characteristic hole-with-dot appearance. Panel E (CT at 6 months post-treatment) shows resolution of cysts and residual punctate calcifications — the classic natural history.
CT findings: Cystic lesion 1–2 cm with thin walls and a 1–3 mm mural nodule (scolex), ring enhancement, calcifications, or hydrocephalus. — Tintinalli's Emergency Medicine
Clinical Manifestations
- Seizures — most common presentation (partial with/without secondary generalization); occur as parasite degenerates and triggers inflammatory response
- Headache — from increased ICP or meningeal irritation
- Focal neurological deficits — depending on cyst location
- Obstructive hydrocephalus — from ventricular/aqueductal cysts → raised ICP, Bruns syndrome (sudden drop attacks with lateral gaze)
- Meningitis/arachnoiditis — subarachnoid NCC
- Vasculitis/stroke — subarachnoid inflammation involving perforating arteries
- Visual disturbance — ocular cysticercosis
In 80–90% of single-cyst parenchymal NCC cases, the lesion resolves within 3–6 months without seizure recurrence. Up to 20% continue to have ongoing seizures. — Tintinalli's Emergency Medicine
Diagnosis
Definitive diagnosis relies on combination of:
- Clinical picture (seizures, headache)
- Exposure/travel history (endemic region, household tapeworm carrier, pig contact)
- Neuroimaging (CT or MRI)
- Serology — Enzyme-Linked Immunotransfer Blot (EITB/Western blot) is the confirmatory test of choice (more specific than ELISA)
Fundoscopic examination is mandatory in all suspected cases to rule out ocular cysticercosis before initiating antiparasitic therapy (antiparasitics can worsen ocular disease). — Harrison's, p. 1181
A negative serologic result does not exclude NCC, especially in single calcified lesions or patients with only 1 cyst (sensitivity is lower). — Red Book 2021
Treatment
Treatment is tailored to the form, location, and viability of cysts (adapted from IDSA/ASTMH 2017 Guidelines): — Bradley and Daroff's Neurology in Clinical Practice, Table 79.7
Parenchymal NCC
| Scenario | Treatment |
|---|---|
| 1–2 viable/degenerating cysts | Albendazole 15 mg/kg/day (÷2 doses) × 10–14 days + corticosteroids |
| >2 viable cysts | Albendazole + Praziquantel (50 mg/kg/day × 10–14 days) + corticosteroids |
| Calcified cysts only | No antiparasitic therapy; treat seizures with AEDs |
| Cysticercal encephalitis (diffuse cerebral edema) | No antiparasitic — steroids only (antiparasitics worsen cerebral edema) |
Steroids (prednisone or dexamethasone) are started before antiparasitic therapy to blunt the host inflammatory response to dying parasites.
Extraparenchymal NCC
| Location | Treatment |
|---|---|
| Intraventricular (accessible) | Neuroendoscopic removal (lateral/3rd ventricle); microsurgical or neuroendoscopic for 4th ventricle |
| Intraventricular (not accessible) | Ventricular shunt → then antiparasitic + steroids |
| Subarachnoid | Shunt if hydrocephalus → prolonged albendazole ± praziquantel + steroids |
| Hydrocephalus, no visible cysts | Ventricular shunt only; no antiparasitic |
| Spinal NCC | Surgical removal or antiparasitic + steroids (individualized) |
| Ocular NCC | Surgical resection — antiparasitics are contraindicated as inflammation can cause permanent vision loss |
Seizure Management
- Anticonvulsant therapy initiated at first seizure; monotherapy usually sufficient
- AEDs can be withdrawn after 24 consecutive seizure-free months AND complete radiological resolution on follow-up CT/MRI
- Long-term AED therapy if seizures persist after lesion resolution/calcification — Harrison's, p. 1181
Case Resolution
CT brain for this patient shows a 1.5 cm ring-enhancing lesion in the right parietal lobe with surrounding edema and a small internal nodule (scolex). EITB serology is positive. Fundoscopy is normal.
Diagnosis: Single colloidal-stage parenchymal neurocysticercosis.
Management:
- Start dexamethasone → then albendazole 15 mg/kg/day × 14 days
- Levetiracetam for seizure control
- Follow-up MRI in 3 months; if lesion resolves and no further seizures, plan AED taper at 24 months
Key Teaching Points
- NCC is the #1 cause of acquired epilepsy worldwide — always consider in a patient from an endemic region with new seizures.
- The "hole-with-dot" sign on MRI (cyst + eccentric scolex) is pathognomonic for viable vesicular stage NCC.
- Do NOT give antiparasitic therapy in: calcified lesions, cysticercal encephalitis with diffuse edema, or ocular NCC.
- Albendazole monotherapy for 1–2 cysts; combination albendazole + praziquantel for >2 cysts.
- Always perform fundoscopy before starting antiparasitics.
- Seronegative EITB does not rule out NCC.
- Intraventricular NCC → neuroendoscopic removal preferred over medical therapy.
Recent evidence (2025): A systematic review and meta-analysis (PMID 40381508) confirms neuroendoscopic management as effective and safe for intraventricular NCC, supporting surgical removal as first-line. A systematic review on movement disorders in NCC (PMID 40822429) highlights an underrecognized presentation spectrum beyond epilepsy.
Sources: Harrison's Principles of Internal Medicine 22E; Bradley and Daroff's Neurology in Clinical Practice; Goldman-Cecil Medicine; Tintinalli's Emergency Medicine; Katzung's Basic and Clinical Pharmacology; IDSA/ASTMH 2017 Guidelines (White et al., Clin Infect Dis 2018)
This is a shared conversation. Sign in to Orris to start your own chat.