Vericose vein
Reading File
Finding Sources
Searching PubMed
"varicose veins"[MeSH Terms] AND treatment
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information. Let me compile the full answer.
Varicose Veins
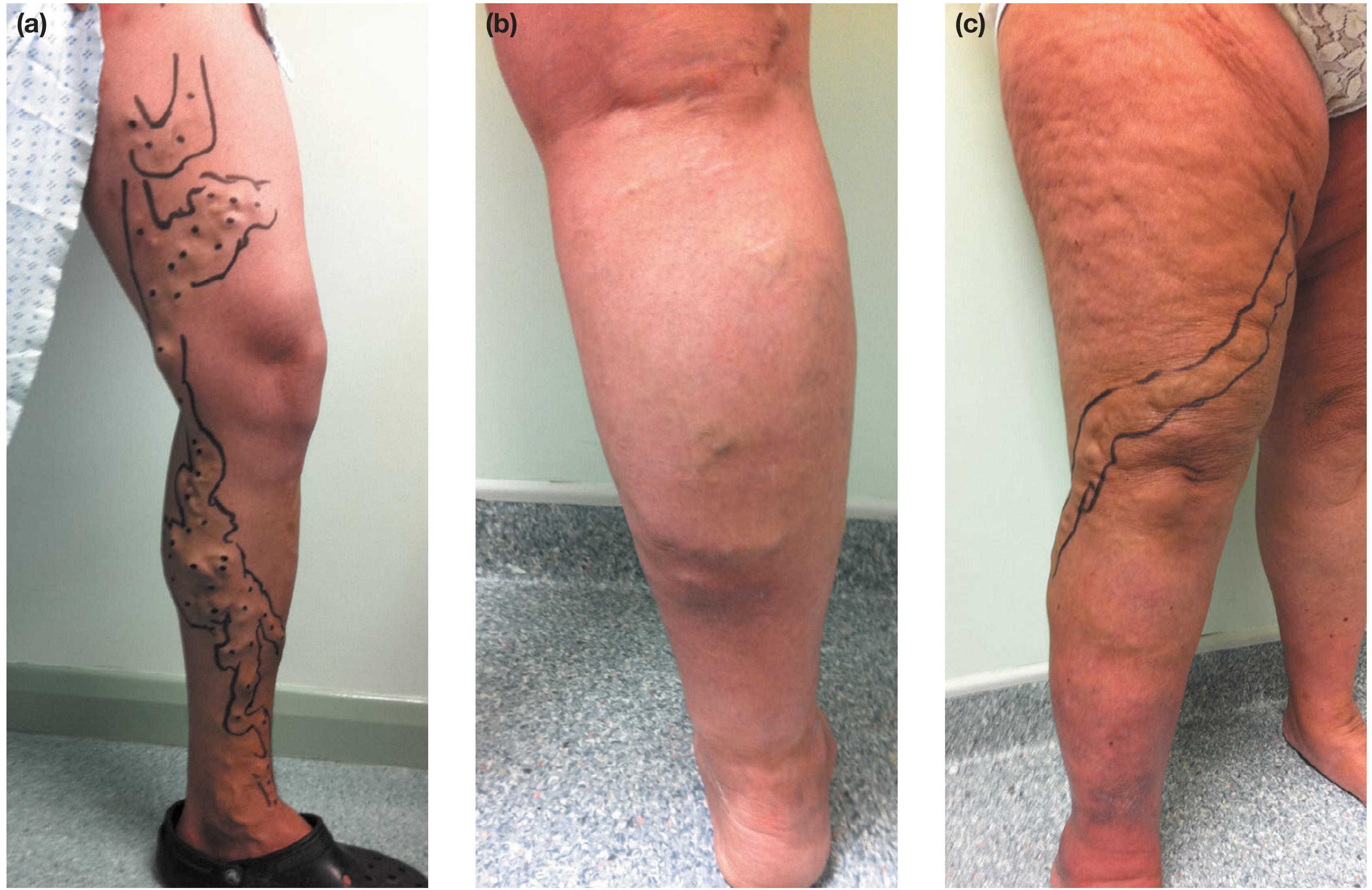
Fig. 62.3 - Bailey and Love: Varicose veins: marked for surgery (a), edema (b), and tortuous veins along the saphenous territory (c).
Definition
Varicose veins are dilated, tortuous superficial veins measuring at least 3 mm in diameter. They most commonly affect the lower limbs. The smaller reticular veins (1-3 mm, blue-green, non-protruding) and telangiectasias (spider veins, <1 mm) are related but distinct entities on the spectrum of chronic venous disease (CVD).
- Harrison's Principles of Internal Medicine 22E, p. 2224
- Gray's Anatomy for Students, p. 44
Epidemiology
- Adult prevalence of visible varicose veins: 30-50% (Bailey & Love); ~15% in men and ~30% in women in the United States (Harrison's).
- Chronic venous insufficiency with edema affects ~7.5% of men and 5% of women.
- ~20% of patients with chronic venous insufficiency develop venous ulcers.
Risk factors:
| Factor | Detail |
|---|---|
| Sex | Higher prevalence in women |
| Age | Prevalence rises sharply with age; from 11.5% (18-24 yr) to 55.7% (55-64 yr) in the Edinburgh Vein Study |
| Pregnancy | Increases risk |
| Family history | Strong familial susceptibility |
| Obesity / tall stature | Higher BMI and height associated |
| Occupation | Prolonged standing (evidence inconclusive) |
- Bailey and Love's Short Practice of Surgery 28th Ed., p. 1052
Anatomy and Pathophysiology
Relevant anatomy:
- Superficial veins: great saphenous vein (GSV) - longest vein in the body, medial side from foot to common femoral vein; small saphenous vein (SSV) - posterolateral calf to popliteal vein.
- Deep veins accompany arteries (tibial, popliteal, femoral, iliac).
- Perforating veins connect the two systems; normally allow flow from superficial to deep only.
Mechanism:
- Venous valves in perforating and axial veins become incompetent.
- This allows retrograde (reflux) blood flow under raised hydrostatic pressure.
- The increased volume and pressure cause progressive dilation and tortuosity of the superficial veins.
- Continued venous hypertension leads to capillary leak, edema, inflammatory cell infiltration, and eventual skin changes (lipodermatosclerosis, pigmentation, ulceration).
Valve incompetence commonly starts at the saphenofemoral junction (SFJ) or saphenopopliteal junction (SPJ), leading to axial reflux down the GSV or SSV respectively.
- Harrison's, p. 2223-2224
- Gray's Anatomy for Students, p. 44
Clinical Features
Symptoms
- Aching, heaviness, throbbing, burning, or bursting sensation in the legs
- Symptoms worsen throughout the day and with prolonged standing
- Relieved by leg elevation and compression hosiery
- Itching (especially with complications)
- Ankle swelling
Signs (on examination - patient standing)
- Visible, distended, tortuous surface veins along the GSV or SSV territory
- Ankle edema (pitting in early stages, later indurated)
- Skin changes:
- Hyperpigmentation (hemosiderin deposition)
- Lipodermatosclerosis - induration + inflammation, just above the ankle
- Atrophie blanche - white scar patches near the medial malleolus
- Stasis eczema/dermatitis
- Phlebectasia corona - fan-shaped intradermal veins near ankle
- Venous ulcer - shallow, irregular border, near medial/lateral malleolus
Complications
-
Chronic: skin changes, venous ulceration
-
Acute: superficial vein thrombosis (thrombophlebitis), bleeding
-
Bailey and Love, p. 1052
-
Harrison's, p. 2224
CEAP Classification
The internationally accepted classification of CVD:
| Class | Description |
|---|---|
| C0 | No visible/palpable signs |
| C1 | Telangiectasias or reticular veins |
| C2 | Varicose veins |
| C2r | Recurrent varicose veins |
| C3 | Edema |
| C4a | Pigmentation or eczema |
| C4b | Lipodermatosclerosis or atrophie blanche |
| C4c | Corona phlebectatica |
| C5 | Healed venous ulcer |
| C6 | Active venous ulcer |
| C6r | Recurrent active venous ulcer |
Etiologic (E): Primary, Secondary, Congenital
Anatomic (A): Superficial, Perforator, Deep
Pathophysiologic (P): Reflux, Obstruction, Both, None
Anatomic (A): Superficial, Perforator, Deep
Pathophysiologic (P): Reflux, Obstruction, Both, None
- Harrison's Table 293-1
Investigations
Duplex Ultrasound (Gold Standard)
- Combines B-mode imaging with spectral/color Doppler
- Identifies reflux (retrograde flow >0.5 sec in superficial/crural veins; >1 sec in proximal deep veins) and obstruction
- Performed with patient standing
- Maps the SFJ/SPJ, full length of GSV/SSV, and perforators
- The "Mickey Mouse" sign on transverse groin scan: GSV and common femoral vein (CFV) medial to common femoral artery (CFA)
Bedside Tests (largely replaced by ultrasound)
- Brodie-Trendelenburg test: tourniquet applied to thigh after elevating leg; fast refilling after tourniquet release = SFJ incompetence; rapid filling before release = deep vein incompetence.
- Perthes test: tourniquet at mid-thigh, patient walks; collapse of below-knee varices indicates competent deep system; distension indicates deep vein obstruction.
Other imaging (rarely needed)
-
MR/CT/conventional venography for IVC/iliofemoral disease, May-Thurner syndrome, post-DVT obstruction.
-
Bailey and Love, p. 1053
-
Harrison's, p. 2224
Treatment
1. Conservative (Supportive) Measures
- Leg elevation periodically, avoid prolonged standing
- Compression hosiery:
- British Class 1: 14-17 mmHg; Class 2: 18-24 mmHg; Class 3: 25-35 mmHg
- 20-30 mmHg suitable for simple varicose veins; 30-40 mmHg for venous ulcers
- Relieves symptoms but does not prevent progression or cure varicose veins
- Poor long-term patient compliance
- Exercise, weight loss, skin care
2. Endothermal Ablation (Current Gold Standard for axial reflux)
Replaced surgical ligation/stripping as first-line treatment. Performed outpatient under local anaesthetic (tumescent anaesthesia). Tumescent anaesthesia compresses the vein onto the device, displaces heat away from nerves, and acts as a heat sink.
| Technique | Mechanism | Notes |
|---|---|---|
| Endovenous Laser Ablation (EVLA) | Laser fibre (1470 nm wavelength) inserted into vein; heat destroys vein wall | ~60-80 J/cm energy delivery; high technical efficacy |
| Radiofrequency Ablation (RFA) | Electromagnetic current heats catheter coil to 120°C for 20-sec cycles (ClosureFast device) | Most evidence-supported RFA device; 3 cm and 7 cm coils available |
Both techniques have equivalent outcomes; RFA may have slightly less postoperative pain/bruising. A 2024 meta-analysis (PMID 38316290) comparing EVLA vs RFA found comparable safety and efficacy profiles.
3. Foam Sclerotherapy
- Sclerosant foam (e.g., sodium tetradecyl sulfate or polidocanol) injected under ultrasound guidance
- Destroys vein endothelium and causes fibrosis
- Used for axial veins, tributaries, residual/recurrent veins, and as an alternative to ablation
- Higher recurrence rates than endothermal ablation
4. Mechanochemical Ablation (MOCA) and Cyanoacrylate Glue
- Newer non-thermal, non-tumescent techniques
- Avoid tumescent injection and thus reduce procedure time/discomfort
- MOCA combines mechanical abrasion with sclerosant
5. Surgical Treatment (where endovenous techniques not suitable)
-
High ligation and stripping (Trendelenburg operation):
- SFJ flush ligation at groin + stripping of GSV to knee
- Stripping below the knee increases sural nerve injury risk
- SPJ ligation + SSV stripping/resection for small saphenous disease
-
Phlebectomy (avulsions):
- Removal of varicose tributaries via multiple small stab incisions using mosquito forceps/phlebectomy hooks
- Can be performed alone under local anaesthetic or combined with axial vein treatment
-
Complication rates: wound infection, haematoma, nerve injury (sural nerve with SSV surgery), DVT, popliteal vein injury
-
Bailey and Love, pp. 1054-1060
-
Harrison's, pp. 2224-2225
-
Schwartz's Principles of Surgery 11th Ed.
Venous Ulcer Management
- Compression bandaging (multilayer) is standard of care
- Wound dressings: low-adherent absorptive (first-line); hydrocolloid, hydrogel, foam, or alginate as alternatives
- Debridement of necrotic tissue
- Antibiotics only if ulcer is infected
- Treat underlying reflux once ulcer healed (reduces recurrence)
Key Points Summary
| Aspect | Key Fact |
|---|---|
| Definition | Tortuous superficial veins ≥3 mm |
| Commonest site | Lower limb GSV territory |
| Primary cause | Valvular incompetence + reflux |
| Gold standard investigation | Duplex ultrasound |
| Gold standard treatment | Endothermal ablation (EVLA or RFA) |
| Classification | CEAP C0-C6 |
| Most serious complication | Venous ulceration |
| Acute complications | Thrombophlebitis, bleeding |
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Ed. (Chapter 62)
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025) (Chapter 293)
- Gray's Anatomy for Students
- Schwartz's Principles of Surgery, 11th Ed.
- Jiang W et al. EVLA vs RFA meta-analysis. J Vasc Surg Venous Lymphat Disord, 2024 Sep (PMID 38316290)
This is a shared conversation. Sign in to Orris to start your own chat.