Give me ecg changed and ecgs of top 10 most common cases
Reading File
Finding Sources
Searching Images
ECG electrocardiogram STEMI ST elevation myocardial infarction
Finding Sources
Searching Images
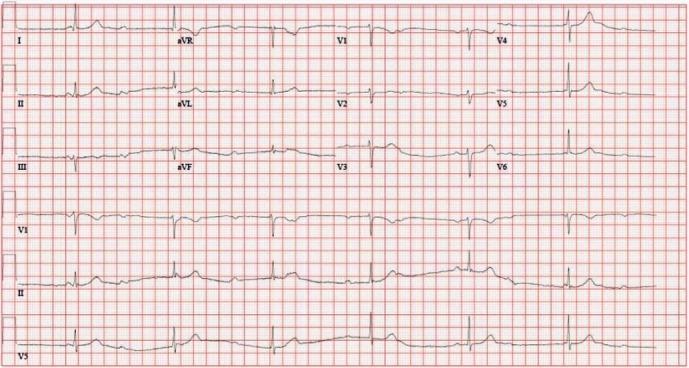
ECG atrial fibrillation irregular rhythm
Searching Images
ECG complete heart block third degree AV block
Searching Images
ECG left bundle branch block LBBB wide QRS
Searching Images
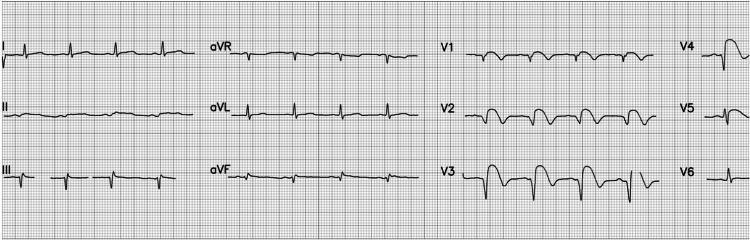
ECG hyperkalemia peaked T waves sine wave
Searching Images
ECG ventricular tachycardia wide complex tachycardia
Searching Images
ECG pulmonary embolism S1Q3T3 right heart strain
Searching Images
ECG Wolff-Parkinson-White WPW delta wave pre-excitation
Searching Images
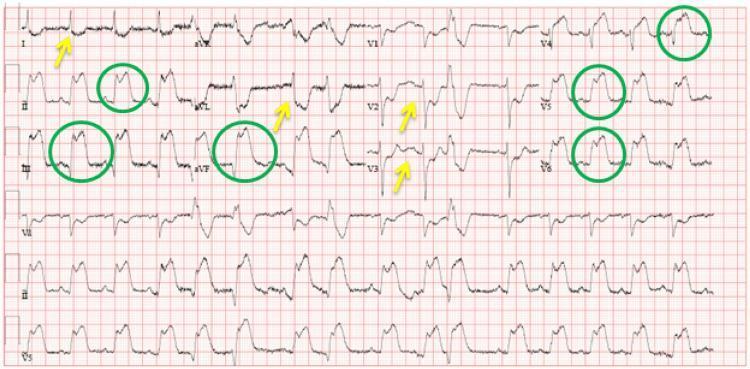
ECG pericarditis diffuse ST elevation saddle shape PR depression
Searching Images
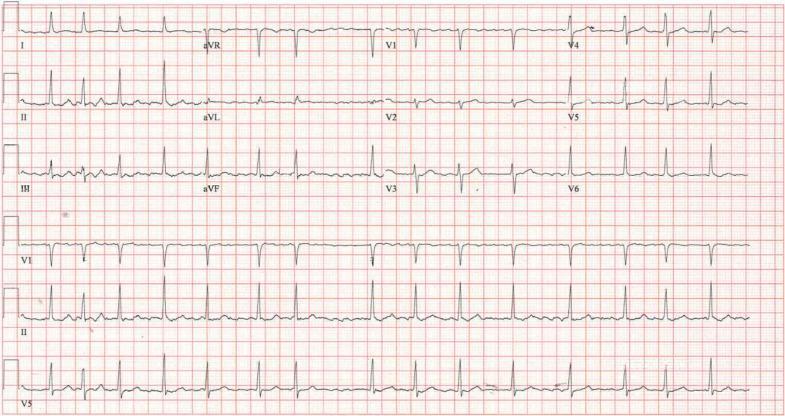
ECG long QT syndrome QTc prolongation torsades de pointes
I now have all the ECGs needed. Here is the comprehensive guide:
Top 10 Most Common ECG Cases — Changes & Tracings
1. 🫀 STEMI (ST-Elevation Myocardial Infarction)
ECG Changes
| Feature | Details |
|---|---|
| ST elevation | ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in ≥2 contiguous precordial leads |
| Reciprocal ST depression | In opposite leads (e.g., inferior STEMI → ST depression in I, aVL) |
| Hyperacute T-waves | Tall, broad, symmetric — earliest sign |
| Pathological Q-waves | Develop later → indicate necrosis (>25% QRS height, >40 ms wide) |
| Tombstoning | Convex/domed ST morphology = high-risk |
Localisation:
- Anterior (V1–V4): LAD occlusion
- Inferior (II, III, aVF): RCA or LCx
- Lateral (I, aVL, V5–V6): LCx
- aVR elevation + widespread depression: Left main / proximal LAD
ECG — Anterior STEMI (Tombstoning, V2–V5)
ECG — Anterolateral STEMI with reciprocal changes

ECG — Inferolateral STEMI (II, III, aVF, V5–V6 elevation)
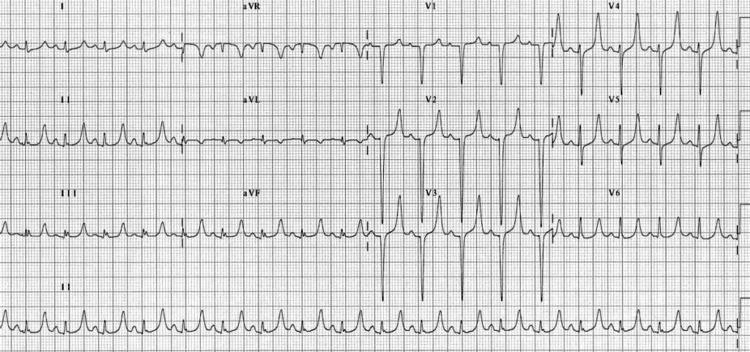
2. 💓 Atrial Fibrillation (AF)
ECG Changes
| Feature | Details |
|---|---|
| No P-waves | Replaced by chaotic fibrillatory (f) waves — best seen in V1 |
| Irregularly irregular R-R intervals | Hallmark feature |
| Narrow QRS | Unless aberrant conduction (e.g., WPW or BBB) |
| Ventricular rate | Variable; rapid if uncontrolled (>100 bpm) |
| f-wave amplitude | Coarse AF (>1 mm) vs. fine AF |
ECG — Classic AF (absent P-waves, irregular RR)
3. 🔵 Complete (Third-Degree) AV Block
ECG Changes
| Feature | Details |
|---|---|
| Complete AV dissociation | P-waves and QRS complexes march independently |
| Regular P-P intervals | Atrial rate > ventricular rate |
| Regular R-R intervals | Escape rhythm is regular |
| Narrow QRS | Junctional escape (~40–60 bpm) |
| Wide QRS | Ventricular escape (<40 bpm) — infra-Hisian block |
| P-waves "march through" | Appear before, within, and after QRS |
ECG — Complete Heart Block (wide QRS ventricular escape, AV dissociation)

ECG — Complete Heart Block (narrow QRS junctional escape)
4. 🟦 Left Bundle Branch Block (LBBB)
ECG Changes
| Feature | Details |
|---|---|
| QRS duration | >120 ms |
| Lead I, aVL, V5–V6 | Broad, notched "M-shaped" R-wave (William pattern) |
| Lead V1 | Deep, wide QS or rS pattern |
| No septal Q-waves | In lateral leads (I, V5–V6) |
| ST/T discordance | T-waves opposite to QRS direction (normal for LBBB) |
| New LBBB | Treat as STEMI-equivalent until proven otherwise (Sgarbossa criteria) |
ECG — Classic LBBB (M-shaped R in I/aVL, deep QS in V1)

5. ⚡ Ventricular Tachycardia (VT)
ECG Changes
| Feature | Details |
|---|---|
| Rate | 100–250 bpm, regular |
| Wide QRS | >120 ms, bizarre morphology |
| AV dissociation | P-waves independent of QRS = diagnostic of VT |
| Capture beats | Narrow QRS amid wide complexes = VT |
| Fusion beats | Intermediate morphology = VT |
| Concordance | All precordial leads positive (positive) or all negative (negative) = VT |
| Northwest axis | Extreme axis deviation (aVR positive) = VT |
ECG — Monomorphic VT (wide complex tachycardia, positive precordial concordance)

6. 🫁 Pulmonary Embolism (PE)
ECG Changes
| Feature | Details |
|---|---|
| Sinus tachycardia | Most common ECG finding in PE |
| S1Q3T3 | S-wave in I, Q-wave in III, T-wave inversion in III |
| T-wave inversions V1–V4 | Right heart strain pattern |
| Incomplete/complete RBBB | Due to RV pressure overload |
| Right axis deviation | RV dilation |
| P pulmonale | Tall peaked P in II (>2.5 mm) |
| AF | Can be precipitated by acute PE |
ECG — PE with S1Q3T3 + sinus tachycardia (annotated)

ECG — PE with S1Q3T3, RBBB, and V1–V4 T-wave inversions

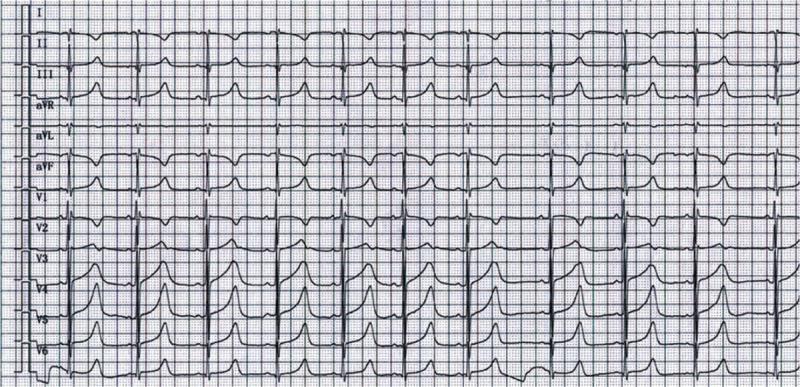
7. ⚗️ Hyperkalemia
ECG Changes (progressive with rising K⁺)
| K⁺ Level | ECG Finding |
|---|---|
| 5.5–6.5 mEq/L | Tall, peaked (tented) T-waves — narrow base, symmetric |
| 6.5–7.0 mEq/L | Flattened/absent P-waves, prolonged PR |
| 7.0–8.0 mEq/L | Wide QRS — intraventricular conduction delay |
| >8.0 mEq/L | Sine-wave pattern → VF/asystole |
ECG — Hyperkalemia (peaked tented T-waves, QRS widening)
ECG — Early Hyperkalemia (classic peaked T-waves, K⁺ 7.3)

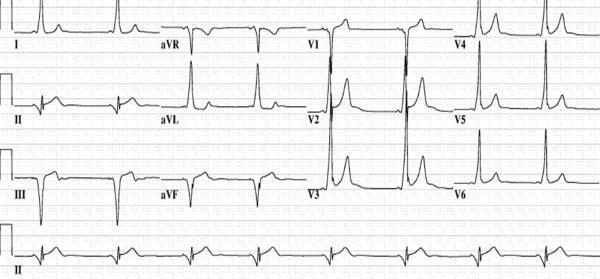
8. 🌩️ Wolff-Parkinson-White (WPW) Syndrome
ECG Changes
| Feature | Details |
|---|---|
| Short PR interval | <120 ms (bypasses AV node delay) |
| Delta wave | Slurred upstroke at start of QRS |
| Wide QRS | >120 ms (fusion of normal + accessory conduction) |
| Secondary ST/T changes | Discordant — opposite to QRS |
| Pseudo-infarct Q-waves | Negative delta waves mimic Q-waves |
| Risk | AF with rapid conduction → VF (avoid AV nodal blockers!) |
Pathway localisation from delta wave polarity:
- Negative delta in II, III, aVF → posteroseptal pathway
- Positive delta in V1 → left lateral pathway
ECG — WPW (short PR, delta wave, wide QRS with annotated accessory pathway)

ECG — WPW (posteroseptal pathway, negative delta in II/III/aVF)
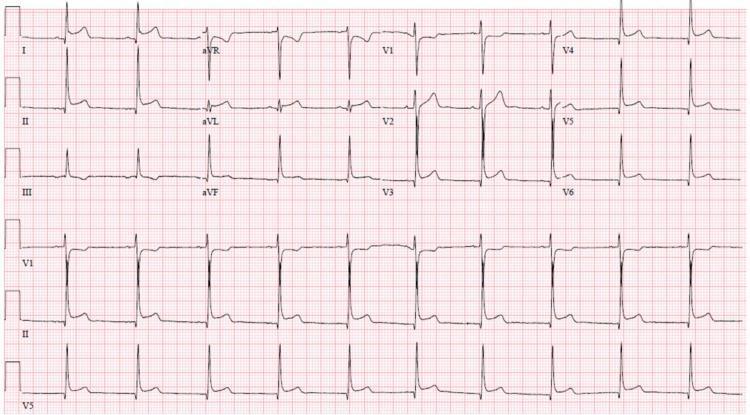
9. 🔴 Acute Pericarditis
ECG Changes (4 stages)
| Stage | Timing | ECG Change |
|---|---|---|
| I | Hours–days | Diffuse concave ST elevation (all leads except aVR/V1); PR depression |
| II | Days | ST normalises; PR still depressed |
| III | Weeks | T-wave inversions develop (without Q-waves) |
| IV | Weeks–months | ECG normalises |
Key distinguishing features from STEMI:
- Diffuse ST elevation (not territory-specific)
- Concave/saddle-shaped ST (vs. convex in STEMI)
- PR depression in II, V4–V6 (PR elevation in aVR)
- No reciprocal ST depression (except aVR and V1)
- Spodick's sign — downsloping TP segment
ECG — Acute Pericarditis (diffuse saddle-shaped STE + PR depression)

ECG — Pericarditis (diffuse STE, PR depression, Spodick's sign annotated)
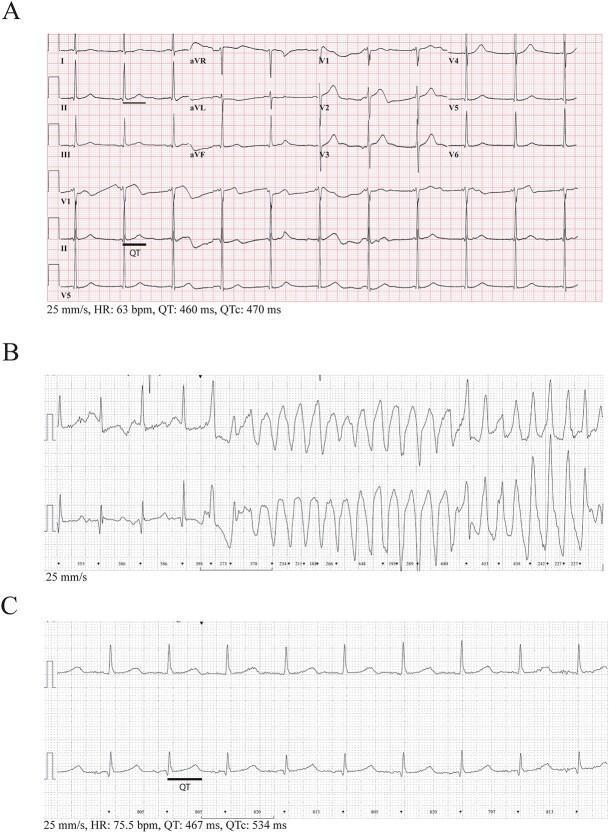
10. ⏱️ Long QT Syndrome (LQTS) / Torsades de Pointes
ECG Changes
| Feature | Details |
|---|---|
| QTc prolongation | Males: >440 ms; Females: >460 ms; Alarming: >500 ms |
| QTc formula | QT / √RR (Bazett); also use Fridericia |
| T-wave morphology by subtype | LQT1: broad-based T; LQT2: notched/bifid T; LQT3: late-onset T with long isoelectric ST |
| Torsades de Pointes | Polymorphic VT with QRS axis "twisting" around the baseline |
| Triggers | Hypokalemia, drugs (antiarrhythmics, antiemetics, antipsychotics), congenital mutations |
ECG — Long QT Syndrome (QTc 514 ms, broad T-waves)
ECG — LQTS with Torsades de Pointes (twisting QRS morphology)
Quick Summary Table
| # | Condition | Key ECG Finding |
|---|---|---|
| 1 | STEMI | ST elevation ≥1 mm in ≥2 leads, reciprocal depression, Q-waves |
| 2 | Atrial Fibrillation | Absent P-waves, irregularly irregular rhythm |
| 3 | Complete AV Block | AV dissociation, regular escape rhythm, P-waves march through QRS |
| 4 | LBBB | QRS >120 ms, M-shaped R in V5–V6, QS in V1, no lateral Q-waves |
| 5 | Ventricular Tachycardia | Wide complex tachycardia, AV dissociation, capture/fusion beats |
| 6 | Pulmonary Embolism | Sinus tach, S1Q3T3, T-wave inversions V1–V4, RBBB |
| 7 | Hyperkalemia | Peaked T-waves → wide QRS → sine wave |
| 8 | WPW Syndrome | Short PR, delta wave, wide QRS |
| 9 | Acute Pericarditis | Diffuse concave STE, PR depression, no reciprocal changes |
| 10 | Long QT / TdP | QTc >500 ms, broad/notched T-waves, polymorphic VT |
This is a shared conversation. Sign in to Orris to start your own chat.