Iron preparation folic acid and b12 pharma
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive pharmacology summary of Iron Preparations, Folic Acid, and Vitamin B12.
Iron Preparations, Folic Acid & Vitamin B12 - Pharmacology
PART 1 - IRON PREPARATIONS
Overview
Iron deficiency is the most common nutritional deficiency worldwide. Iron is stored as ferritin in intestinal mucosal cells, liver, spleen, and bone marrow, and is transported to the marrow by transferrin for hemoglobin production. - Lippincott Illustrated Reviews: Pharmacology, 16th Ed.
Causes of iron deficiency:
- Acute or chronic blood loss
- Menstruation / pregnancy
- Accelerated growth in children
- Malabsorption
Signs: Pica (craving for ice, dirt, paper), koilonychia (spoon nails), angular stomatitis - in addition to the usual anemia symptoms.
Mechanism of Action
Supplementation with elemental iron corrects the deficiency. In the stomach, acidic conditions keep iron in the reduced ferrous (Fe²+) form, which is the more soluble, absorbable form. Iron is then absorbed primarily in the duodenum. The amount absorbed is regulated by body stores - when stores are low, absorption increases; when adequate, absorption decreases.
Oral Iron Formulations
| Formulation | Brand Example | Elemental Iron (%) | Notes |
|---|---|---|---|
| Ferrous gluconate | Fergon, Ferro-Tab | 12% | Less elemental iron; similar tolerability to ferrous sulfate |
| Ferric ammonium citrate | Iron citrate | 18% | Less bioavailable; must be reduced to ferrous form first |
| Ferrous sulfate | Fer-in-Sol, Feratab | 20% | Most common oral iron supplement; low cost |
| Ferrous sulfate, anhydrous | Slow-Fe | 30% | Extended-release; once-daily dosing |
| Ferrous fumarate | Ferretts, Ferrimin | 33% | Similar efficacy to ferrous sulfate; minimal taste |
| Carbonyl iron | Icar, Feosol | 100% | Microparticles; slower absorption = less toxic; releases over 1-2 days |
| Polysaccharide-iron complex | NovaFerrum, Nu-Iron 150 | 100% | Tasteless, odorless; once-daily dosing |
- Lippincott Illustrated Reviews: Pharmacology, 16th Ed., p. 1477
Dosing (CDC recommendation): 60-120 mg/day elemental iron in divided doses 2-3 times daily. Note: Newer evidence shows lower doses (40-80 mg/day) or every-other-day dosing can be equally effective with fewer side effects.
Parenteral Iron Formulations
Used when patients cannot tolerate or absorb oral iron, or in patients on erythropoietin with hemodialysis.
| Agent | Key Features |
|---|---|
| Iron dextran | Highest anaphylaxis risk; requires test dose; IM or IV; IM use now discouraged due to local reactions |
| Sodium ferric gluconate | ~295 kDa; 80% delivered to transferrin within 24 h; lower anaphylaxis risk than iron dextran; used in hemodialysis |
| Iron sucrose | 100-200 mg IV daily over 14 days; total dose 1000 mg; FDA-approved for CKD |
| Ferric carboxymaltose | Up to 1000 mg in 15 min; ~80% distributed to marrow, liver, spleen; FDA-approved for IDA |
| Iron isomaltoside (ferric derisomaltose) | Linear unbranched carbohydrate; theoretically lower immunogenicity |
Important: A test dose must be administered before any parenteral iron. Iron is essential for bacterial growth, so IV iron should be used cautiously in active infections. - Goodman & Gilman's Pharmacological Basis of Therapeutics
Adverse Effects of Oral Iron
- GI disturbances: abdominal pain, constipation, nausea, diarrhea (local irritation)
- Dark stools (harmless)
Monitoring Response
- Reticulocyte count rises in 4-7 days
- Hemoglobin rise measurable after ~4 weeks (target: +2 g/dL or more)
- If no response in 3-4 weeks, reconsider diagnosis
PART 2 - FOLIC ACID (Folate)
Role in Erythropoiesis
Folic acid provides essential methyl group donors for synthesis of amino acids, purines, and DNA. Deficiency leads to failure of nuclear maturation, producing megaloblastic anemia (large, fragile macrocytes with shortened lifespan of 1/2 to 1/3 normal). - Guyton & Hall Medical Physiology
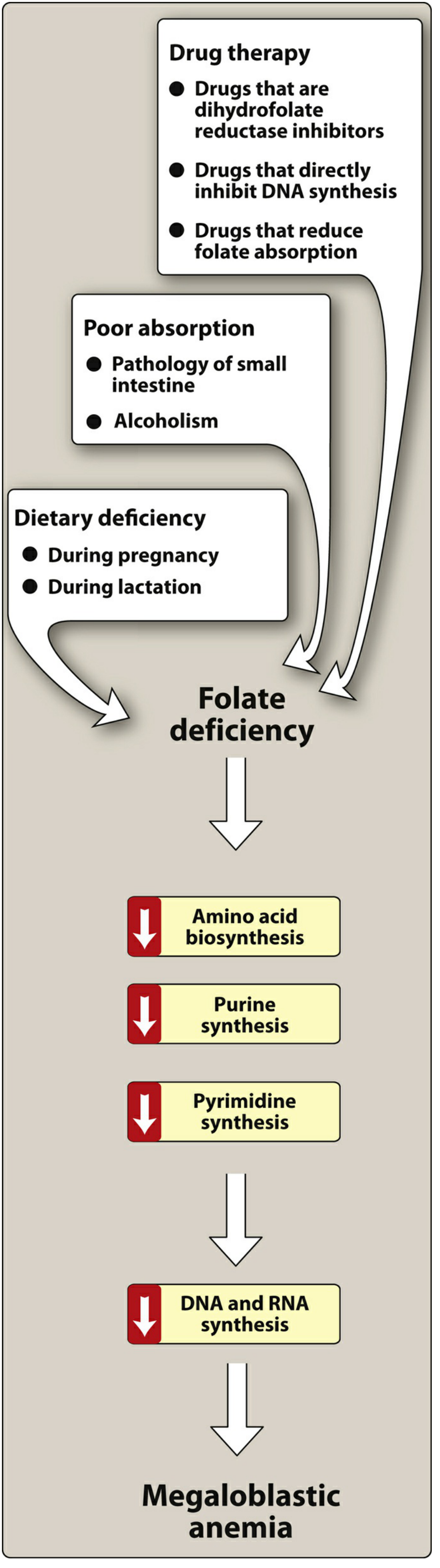
Causes of Folate Deficiency
- Increased demand - pregnancy, lactation
- Poor absorption - small intestinal pathology, alcoholism
- Drug-induced:
- DHFR inhibitors: methotrexate, trimethoprim
- Drugs that directly inhibit DNA synthesis: azathioprine, zidovudine
- Drugs reducing folate absorption: phenytoin, phenobarbital
Pharmacokinetics
- Absorbed rapidly in the jejunum
- Oral administration: well absorbed; parenteral rarely needed
- Excess excreted in urine (nontoxic in overdose)
- Rare hypersensitivity to parenteral injections
Dosing (Harriet Lane Handbook)
| Population | Dose |
|---|---|
| Infant | 0.1 mg/day |
| Child <4 yr | 0.1-0.3 mg/day |
| Child ≥4 yr & adolescent | 0.1-0.4 mg/day |
| Adult | 0.4 mg/day |
| Pregnant / lactating | 0.8 mg/day |
| Women planning pregnancy | 0.4 mg/day before and during pregnancy (NTD prevention) |
Key Clinical Warning
Folic acid can mask the hematologic signs of vitamin B12 deficiency - it corrects the anemia but does NOT prevent the irreversible neurologic damage of B12 deficiency. This is why empiric treatment of megaloblastic anemia should NEVER use folic acid alone, but always with B12 until results are confirmed.
Drug interaction: High-dose folic acid may decrease absorption of phenytoin.
Public Health Role
Since 1998, folic acid fortification of enriched grains in the US/Canada has reduced neural tube defects (spina bifida, anencephaly) by ~20-25%. It also reduces hyperhomocysteinemia (by enabling conversion of homocysteine to methionine via N5-methyltetrahydrofolate), which reduces risk of ischemic heart disease and stroke. - Katzung's Basic & Clinical Pharmacology, 16th Ed.
PART 3 - VITAMIN B12 (Cyanocobalamin / Hydroxocobalamin)
Role in Erythropoiesis
B12 is required for the synthesis of thymidine triphosphate, a building block of DNA. Without it, erythropoietic cells cannot proliferate, producing macrocytes (megaloblasts) with a shortened lifespan. Daily requirement: only 1-3 mcg/day; total body stores ~1000 days' worth. Therefore, 3-4 years of defective absorption are needed before anemia develops. - Guyton & Hall Medical Physiology
Causes of B12 Deficiency
- Pernicious anemia (most common): atrophic gastric mucosa fails to produce intrinsic factor (IF) from parietal cells
- IF binds B12, protects it from digestion, and mediates its absorption via specific receptors in the terminal ileum
- Gastric resection
- Malabsorption syndromes (e.g., sprue)
- Bariatric surgery
- Low dietary intake (strict vegans)
Clinical Features (beyond anemia)
- Tingling / paresthesias in hands and feet
- Difficulty walking (subacute combined degeneration of spinal cord)
- Dementia
- In severe cases: hallucinations, paranoia, schizophrenia
Pharmacokinetics & Formulations (Harriet Lane Handbook)
| Formulation | Details |
|---|---|
| Oral tabs (OTC) | 100, 250, 500, 1000 mcg |
| Sublingual tabs | 2500 mcg |
| Sublingual liquid | 3000 mcg/mL |
| Lozenges (OTC) | 50-500 mcg |
| Nasal spray (Nascobal) | 500 mcg/spray |
| Injection (IM/deep SC) | 1000 mcg/mL |
Preferred parenteral form: Hydroxocobalamin - rapid response, highly protein-bound, longer plasma levels than cyanocobalamin. - Lippincott Illustrated Reviews: Pharmacology
Dosing
Children (IM or deep SC):
- 100 mcg/day x 10-15 days, then 100 mcg once or twice weekly for several months
- Maintenance: at least 60 mcg/month
Adults (IM or deep SC):
- 100 mcg/day x 6-7 days; then every 3-4 days x 2-3 weeks; then monthly maintenance
Oral route: Used for dietary deficiencies (not pernicious anemia). In bariatric surgery patients: daily sublingual cyanocobalamin or monthly IM.
Pernicious anemia: Therapy must be continued for life.
Distinguishing B12 vs. Folate Deficiency (Megaloblastic Anemia Workup)
| Finding | Folate Deficiency | B12 Deficiency |
|---|---|---|
| Serum folate | Low | Normal |
| Serum B12 | Normal | Low |
| Methylmalonic acid (MMA) | Normal | Elevated |
| Homocysteine | Elevated | Elevated |
| Neurologic signs | Absent | Present (subacute combined degeneration) |
Key rule: If MMA is normal but homocysteine is high → folate deficiency. If both MMA and homocysteine are elevated → B12 deficiency (folate deficiency cannot be ruled out). - Lippincott Illustrated Reviews: Pharmacology, Clinical Application 44.3
Summary Comparison Table
| Feature | Iron | Folic Acid | Vitamin B12 |
|---|---|---|---|
| Deficiency anemia type | Microcytic, hypochromic (IDA) | Megaloblastic | Megaloblastic |
| Primary absorption site | Duodenum | Jejunum | Terminal ileum (via IF) |
| Preferred oral form | Ferrous sulfate | Pteroylglutamic acid | Cyanocobalamin |
| Preferred parenteral | Ferric carboxymaltose / iron sucrose | Rare (IM folic acid available) | Hydroxocobalamin (IM) |
| Special concern | GI side effects; anaphylaxis (IV) | Masks B12 deficiency neurologically | Must treat for life in pernicious anemia |
| Pregnancy dose | 30-60 mg elemental iron/day | 0.8 mg/day | Adequate intake required |
This is a shared conversation. Sign in to Orris to start your own chat.