Teach me all 4 types of hypersensitivity reactions in a way i never forgot or confused in this concept
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have everything I need. Let me compile the complete, memorable teaching response.
The 4 Types of Hypersensitivity Reactions - Never Confused Again
Here is the single most powerful anchor to remember them all:
"I Caught A Cold" = IgE → Cytotoxic → Antigen-antibody complex → Cell-mediated = Types I, II, III, IV
And the one master rule: Types I-III are antibody-driven. Type IV is the only one that is purely T cell-driven (no antibody involved). This alone eliminates half the confusion.
The Big Picture Table (Coombs & Gell Classification)
| Feature | Type I | Type II | Type III | Type IV |
|---|---|---|---|---|
| Nickname | Immediate / Anaphylactic | Cytotoxic | Immune Complex | Delayed / Cell-mediated |
| Key player | IgE | IgG or IgM | IgG | T cells (CD4/CD8) |
| Effectors | Mast cells, basophils, eosinophils | Complement, phagocytes, NK cells | Complement, neutrophils, phagocytes | Macrophages, CTLs |
| Timing | Minutes (immediate) + 2-24h (late phase) | Minutes-hours | Hours-days | 48-72 hours |
| Where antigen sits | Soluble/inhaled/injected | On a cell surface | In circulation → deposits | In tissues |
| Key examples | Anaphylaxis, asthma, hay fever, hives | Hemolytic anemia, Goodpasture, Myasthenia gravis | SLE, serum sickness, Arthus reaction | Contact dermatitis, TB, Type 1 DM |
- Robbins & Kumar, Pathologic Basis of Disease (Table 6.1)
TYPE I - Immediate Hypersensitivity (IgE)
The Core Story
Sensitization first, then bang. A person is exposed to an allergen → Th2 cells drive IgE production → IgE coats mast cells via Fc receptors (like loading a gun). On re-exposure, allergen cross-links two IgE molecules on the mast cell surface → mast cell degranulates explosively.
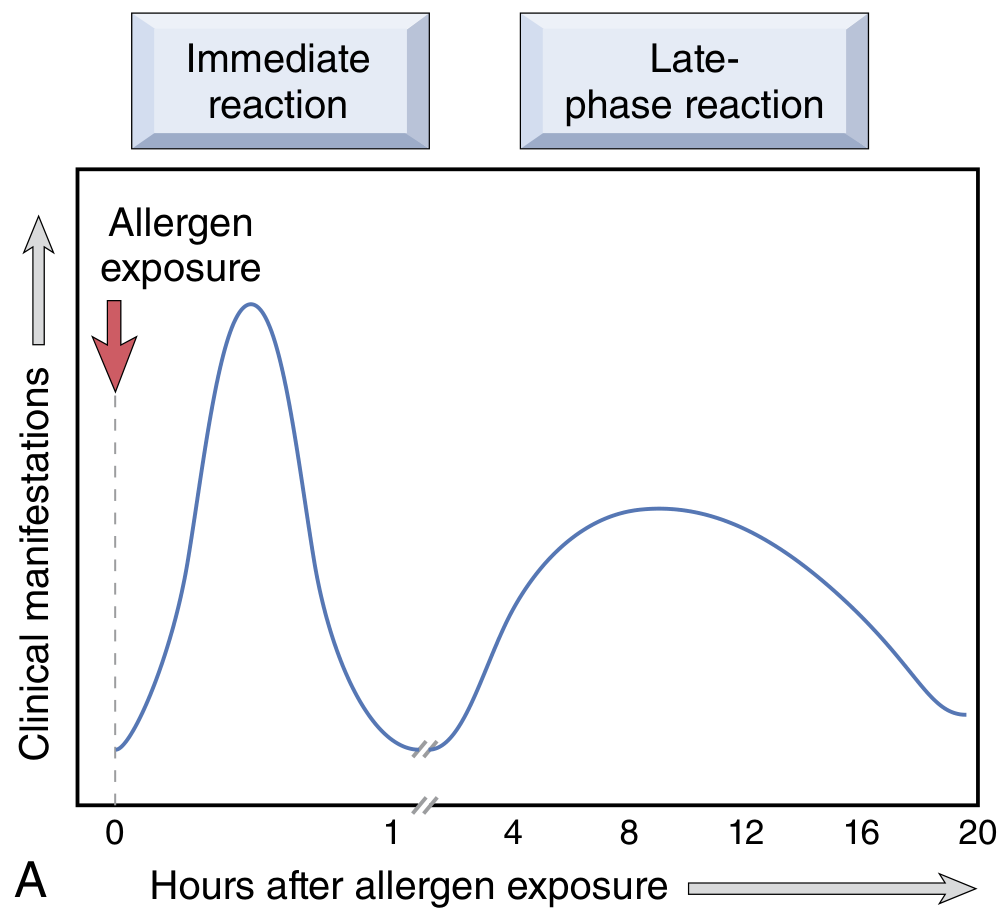
The Two Phases
Phase 1 - Immediate (minutes): Preformed granule contents released:
- Histamine → vasodilation, increased permeability, bronchospasm
- Tryptase/chymase (enzymes) → tissue damage, kinin generation
- Heparin → anticoagulant
Phase 2 - Late (2-24 hours later, no new allergen needed):
- Newly synthesized leukotrienes C4 & D4 → 1000x more potent than histamine for bronchospasm
- Prostaglandin D2 → intense bronchospasm + mucus hypersecretion
- Cytokines (IL-4, IL-5, TNF) → recruit eosinophils and T cells
- Eosinophils arrive and dump major basic protein and eosinophil cationic protein → tissue damage
The late phase is why asthma is chronic, not just a quick wheeze.
Memory Anchor
Type I = "IgE loads the Mast Cell GUN. Allergen pulls the trigger."
-
The cytokine driver is Th2 (IL-4, IL-5, IL-13)
-
Classic mnemonics for diseases: ABCDE = Anaphylaxis, Bronchial asthma, Conjunctivitis, Dermatitis (atopic eczema), Eczema/food allergy
-
Robbins & Kumar, p. 199-201
TYPE II - Antibody-Mediated Cytotoxic Hypersensitivity (IgG/IgM)
The Core Story
Antibody targets something on a cell surface or in tissue matrix and destroys it. The key distinction from Type III: the antigen is cell-bound (not floating free in circulation).
Three Destruction Mechanisms (all from Robbins)
1. Opsonization + Phagocytosis:
IgG coats the cell → macrophage Fc receptors grab it → phagocytosis and destruction.
OR IgM/IgG activates complement → C3b deposits → phagocytosis via C3b receptors.
Complement also assembles the Membrane Attack Complex (MAC) → drills holes → osmotic lysis.
Example: Autoimmune hemolytic anemia, Rh incompatibility
2. ADCC (Antibody-Dependent Cell-Mediated Cytotoxicity):
IgG-coated cell is recognized by NK cells and macrophages via Fc receptors → lysis without phagocytosis.
Example: Some drug-induced cytopenias
3. Cellular Dysfunction (no cell killing, just malfunction):
Antibody blocks or overstimulates a receptor.
- Myasthenia gravis - Anti-ACh receptor antibody blocks neuromuscular transmission → muscle paralysis
- Graves' disease - Anti-TSH receptor antibody stimulates the receptor → hyperthyroidism (antibody acts as a TSH mimic)
- Pernicious anemia - Anti-intrinsic factor antibody → blocks B12 absorption
Memory Anchor
Type II = Antibody attacks a cell's ID (surface antigen). "Cell is WANTED, antibody is the bounty hunter." Key diseases: Goodpasture, Graves, Myasthenia Gravis - all the "G"s + M start with antibody to a specific surface target.
- Robbins & Kumar, p. 202-204
TYPE III - Immune Complex-Mediated Hypersensitivity (IgG)
The Core Story
The antigen is NOT on a cell - it is floating in the blood. Antibody binds it there, forming immune complexes that get deposited in tissues (vessels, glomeruli, synovium) and trigger inflammation from within the wall, not on a cell surface.
The critical pathophysiology:
- Excess antigen + antibody (IgG) → soluble immune complexes form in circulation
- Complexes deposit in vessel walls, glomerular basement membranes, synovial joints
- Complement activation → C3a + C5a (anaphylatoxins + chemotaxins) → neutrophil recruitment
- Neutrophils try to phagocytose embedded complexes but cause "frustrated phagocytosis" → dump lysosomal enzymes into the tissue → fibrinoid necrosis and vasculitis
Two Classic Patterns
Arthus Reaction (local): Inject antigen subcutaneously into a sensitized person → local immune complex deposition → intense acute inflammation at that site within hours. A "model" reaction, rarely clinically significant alone.
Serum Sickness (systemic): Happens 7-10 days after large foreign antigen exposure (e.g., horse anti-venom, some antibiotics). Complexes deposit everywhere → fever, urticaria, arthralgias, glomerulonephritis, lymphadenopathy.
Memory Anchor
Type III = "Immune complexes are like garbage in the pipes." They don't destroy cells directly - they clog small vessels and call in neutrophils who wreck the pipes trying to clean up. Histology shows fibrinoid necrosis (a pink smudgy deposit) in vessel walls. Classic diseases: SLE, serum sickness, post-streptococcal glomerulonephritis, Arthus reaction
- Robbins & Kumar, p. 204-207
TYPE IV - Cell-Mediated (Delayed-Type) Hypersensitivity - T Cells Only
The Core Story
No antibody. No B cells. Pure T cell business. This is the "slow burn" - takes 48-72 hours because T cells need time to traffic to the site and orchestrate inflammation. There are two main T cell subtypes doing the damage:
Subtype A - CD4+ T cell-mediated (Th1 and Th17):
- Sensitized CD4+ T cells recognize antigen → release IFN-γ → macrophage activation → macrophage releases TNF, IL-12, toxic radicals → tissue destruction
- When this goes on chronically with poorly degradable antigens → granuloma formation (epithelioid macrophages + Langhans giant cells + lymphocytic cuff)
- Classic examples: Tuberculin PPD test, contact dermatitis (poison ivy), granulomatous diseases (TB, sarcoidosis, Crohn's disease)
Subtype B - CD8+ CTL-mediated:
- Cytotoxic T lymphocytes directly kill antigen-bearing target cells
- Classic examples: Type 1 Diabetes Mellitus (CD8 cells kill beta cells), viral hepatitis, graft rejection
Classic Clinical Tests
- Mantoux/PPD test: Intradermal injection of tuberculin → if sensitized, induration (not just redness) appears at 48-72 hours = Type IV reaction. The hard bump is the granulomatous T cell response.
- Patch test: For contact dermatitis - apply allergen to skin, read at 48 hours.
Memory Anchor
Type IV = "Delayed, so T cells have to DRIVE to the scene. No fast-response antibody here." The "D" double-meaning: Delayed + DTH (Delayed-Type Hypersensitivity). Granuloma = the signature lesion when macrophages can't clear the insult.
- Robbins & Kumar, p. 207-210; K.J. Lee's Essential Otolaryngology
The Common Confusion Points - Sorted Out
| Confusion | Answer |
|---|---|
| Type II vs Type III - both use IgG? | Type II: antigen is ON a cell surface. Type III: antigen is floating in the blood, complexes deposit in tissues. |
| Which types use complement? | Types II and III both activate complement heavily. Type I uses complement minimally. Type IV: no complement (no antibody). |
| Which is the only "delayed" one? | Type IV only. All others are antibody-mediated and fast (minutes to hours). |
| Myasthenia gravis vs Lambert-Eaton? | Both Type II, both block neuromuscular junction but at different sites. |
| SLE - which type? | Primarily Type III (immune complexes) but also has Type II features (anti-RBC, anti-platelet antibodies). |
| Tuberculin test vs anaphylaxis? | TB = Type IV (48-72h, T cells). Anaphylaxis = Type I (minutes, IgE/mast cells). |
Master Mnemonic - "ACID"
| Letter | Type | Key player |
|---|---|---|
| Anaphylactic | I | IgE + Mast cells |
| Cytotoxic | II | IgG/IgM on cell surfaces |
| Immune complex | III | IgG in circulation → deposits |
| Delayed | IV | T cells only |
ACID - because hypersensitivity reactions are immunologic damage to the body's own tissues, like acid burning from the inside.
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (Table 6.1, Ch. 6, pp. 198-210); Scott-Brown's Otorhinolaryngology (Table 14.1); Cellular and Molecular Immunology; K.J. Lee's Essential Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.