Chest pain and approach to acs acc to harrison with defination
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent — I now have everything needed for a comprehensive answer. Let me compile this into a well-structured response from Harrison's 22nd Edition.
Chest Pain & Approach to ACS — Harrison's Principles of Internal Medicine, 22nd Edition (2025)
1. DEFINITION — Ischemic Heart Disease & ACS
Ischemic heart disease (IHD) is a condition in which there is an inadequate supply of blood and oxygen to a portion of the myocardium; it typically occurs when there is an imbalance between myocardial oxygen supply and demand. The most common cause is atherosclerotic disease of an epicardial coronary artery sufficient to cause a regional reduction in myocardial blood flow.
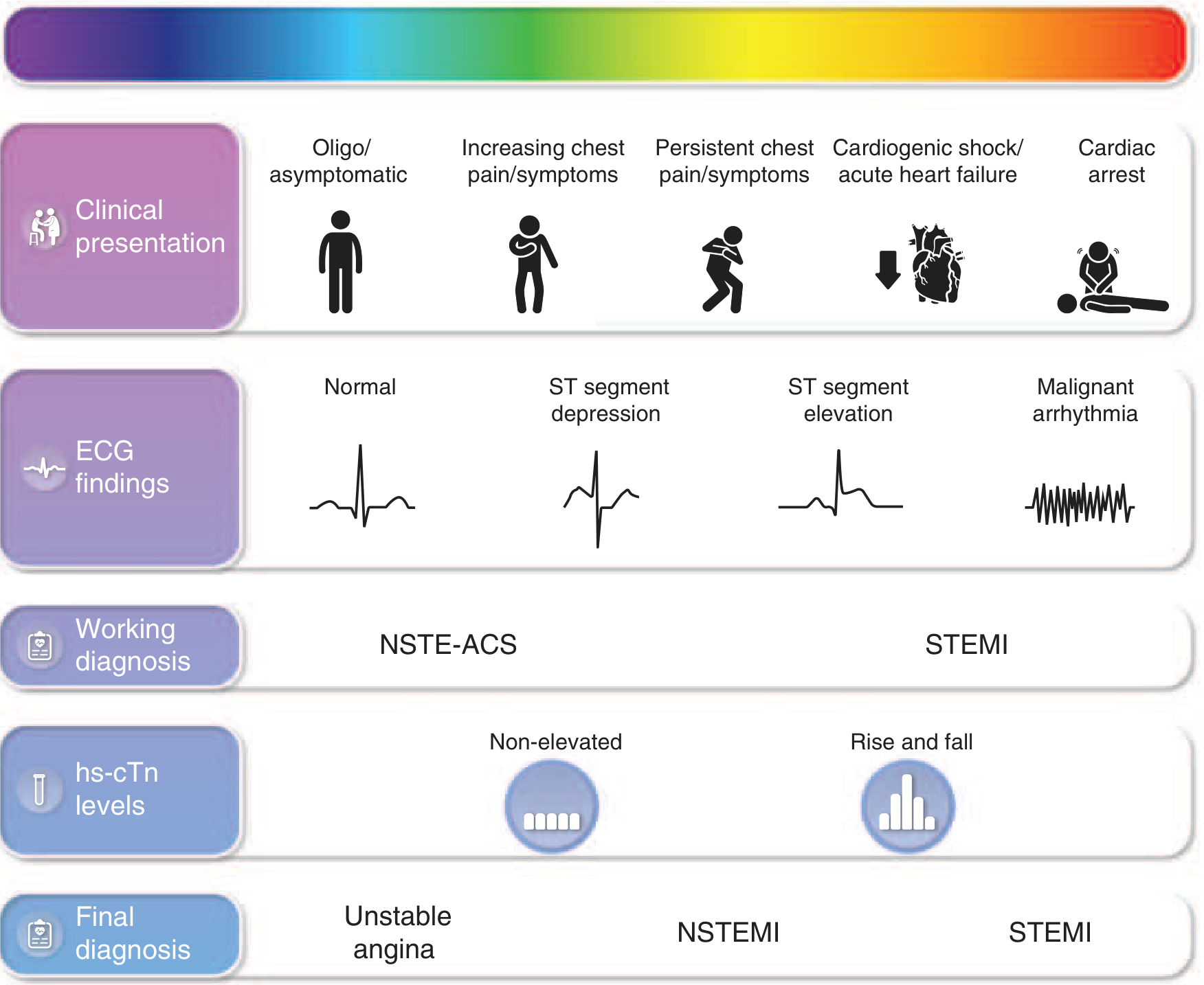
Acute Coronary Syndrome (ACS) is an umbrella term encompassing the acute manifestations of IHD caused by abrupt reduction in coronary blood flow, most commonly from atherothrombotic plaque disruption (rupture or erosion). It spans three diagnoses:
| Final Diagnosis | ECG | Biomarkers (hs-cTn) |
|---|---|---|
| Unstable Angina (UA) | No ST elevation | Non-elevated |
| NSTEMI | No ST elevation (± ST depression/T-wave changes) | Rise and fall (elevated) |
| STEMI | ST elevation | Rise and fall (elevated) |
Harrison's, p. 2150 — FIGURE 285-1 (Spectrum of ACS)
2. CHEST PAIN — Characteristics of Angina Pectoris
The typical patient is a man >50 years or a woman >60 years:
- Quality: Heaviness, pressure, squeezing, smothering, or choking — rarely frank pain
- Location: Central, substernal — patient places a clenched fist over the sternum (Levine's sign)
- Radiation: Either shoulder, both arms (especially ulnar aspects), back, interscapular region, root of neck, jaw, teeth, epigastrium
- Duration: Typically 2–5 minutes; crescendo-decrescendo pattern
- Triggers: Exertion (exercise, hurrying, sexual activity), emotion (stress, anger, fright)
- Relief: Rest, nitroglycerin
- Key negative: Does not radiate to the trapezius (that pattern suggests pericarditis)
- Anginal equivalents (especially in women, elderly, diabetics): dyspnea, epigastric discomfort, nausea, weakness, diaphoresis
Harrison's, p. 2136
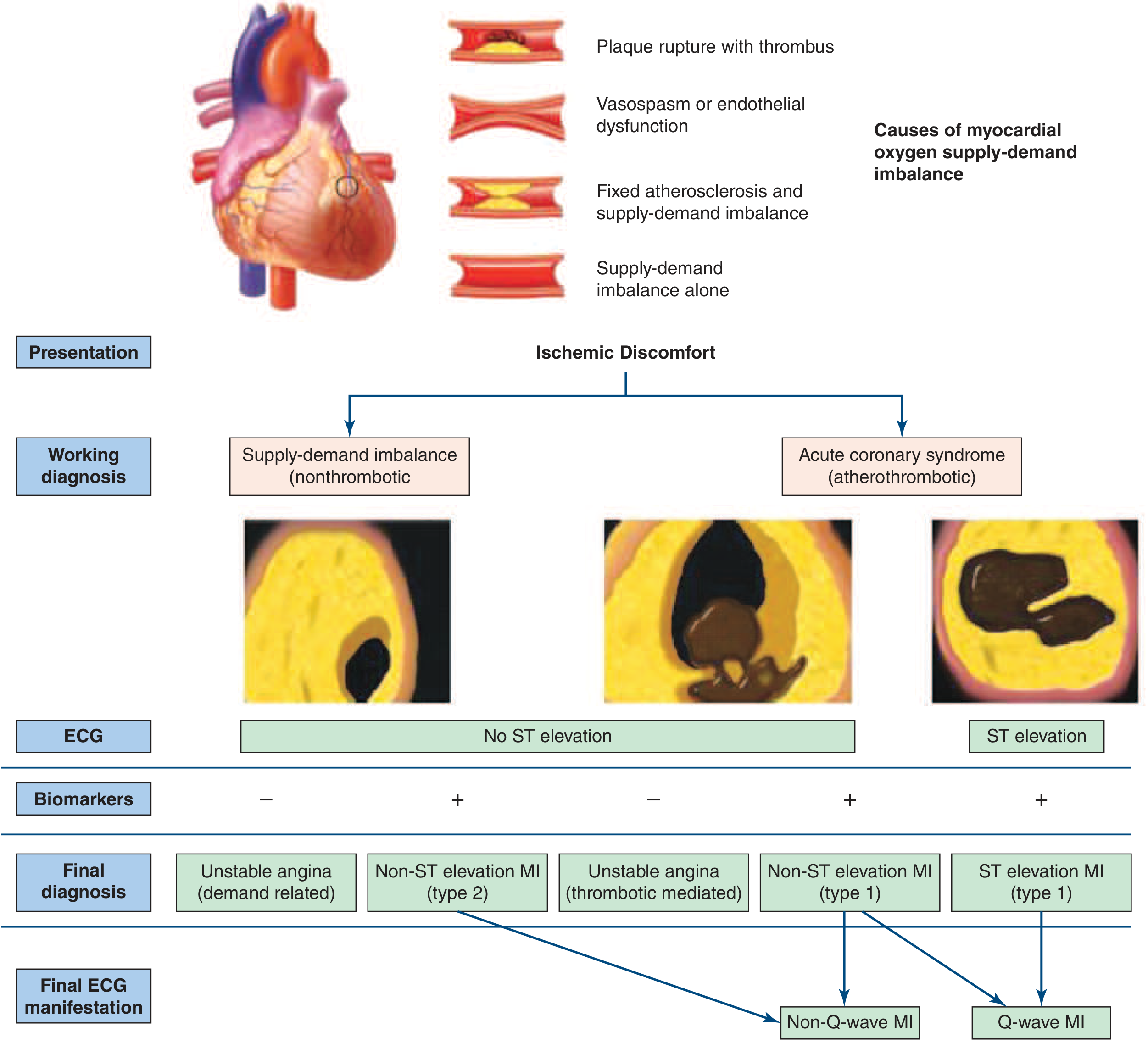
3. PATHOPHYSIOLOGY OF ACS
ACS follows plaque disruption — either rupture (thin fibrous cap, lipid-rich core) or erosion — leading to:
- Platelet adhesion → activation → thromboxane A₂ release → vasoconstriction
- GP IIb/IIIa receptor activation → fibrinogen cross-linking → platelet aggregation
- Tissue factor exposure → coagulation cascade → thrombin → fibrin → thrombus
The final occlusion determines outcome:
- Complete occlusion → STEMI
- Partial/incomplete occlusion → NSTE-ACS (UA or NSTEMI)
4. APPROACH TO ACS — NSTE-ACS (UA & NSTEMI)
Clinical Features (History & Physical)
Chest discomfort in NSTE-ACS has at least one of:
- Occurrence at rest (or minimal exertion), lasting >10 min
- Relatively recent onset (within prior 2 weeks)
- Crescendo pattern — more severe, prolonged, or frequent than previous episodes
Physical examination may show: diaphoresis, pale cool skin, sinus tachycardia, S3/S4, basilar rales, hypotension, or cardiogenic shock in severe cases.
Always rule out life-threatening mimics: pulmonary embolism, aortic dissection, cardiac tamponade.
Risk Stratification
Key high-risk markers:
- Age ≥65 years
- Known CAD (≥50% stenosis)
- ST deviation >0.5 mm on presenting ECG
- Elevated cardiac biomarkers (hsTn)
- ≥2 ischemic episodes in prior 24 h
- ≥3 CAD risk factors
Investigations
- ECG: Serial 12-lead; look for ST depression, T-wave inversions
- hsTn: At presentation, 1 h, and if needed at 3 h — rise/fall pattern confirms NSTEMI
- Stress testing or CT coronary angiography for intermediate-risk patients with diagnostic uncertainty
- Continuous ECG monitoring for ST deviation and arrhythmias
5. TREATMENT — NSTE-ACS
Anti-Ischemic (Acute Phase)
| Drug | Key Points | Avoid When |
|---|---|---|
| Nitrates | SL/buccal 0.3–0.6 mg q5 min × 3; then IV NTG 5–10 μg/min (titrate to relief or SBP <90) | PDE-5 inhibitor use (sildenafil/vardenafil within 24 h; tadalafil within 48 h); hypotension; RV infarction |
| Beta-blockers | Reduce MVO₂; IV for severe ischemia | Acute/severe HF, low output, severe bradycardia, high-degree AV block |
| Oxygen | Only if SpO₂ <90%, HF present | Routine use not indicated |
Antithrombotic Therapy
- Aspirin 325 mg loading → 75–100 mg maintenance
- P2Y₁₂ inhibitor (ticagrelor preferred over clopidogrel in most)
- Anticoagulation: UFH, enoxaparin, fondaparinux, or bivalirudin depending on strategy
Invasive vs. Conservative Strategy
- Early invasive (angiography within 24 h): for high-risk features — elevated hsTn, dynamic ECG changes, TIMI/GRACE score elevation
- Conservative/selective invasive: for low-risk, negative biomarkers, no ECG changes
6. STEMI — Key Additional Points
STEMI occurs when a completely occlusive thrombus forms rapidly at a disrupted plaque site. Management priorities:
- Immediate reperfusion is the goal — primary PCI preferred (door-to-balloon ≤90 min at PCI-capable center)
- Fibrinolysis if primary PCI unavailable within 120 min of first medical contact
- Same antithrombotic backbone (aspirin + P2Y₁₂ + anticoagulation)
7. UNIVERSAL DEFINITION OF MI (Harrison's / Fourth Universal Definition 2018)
Myocardial Injury: Elevated cTn with at least one value above 99th percentile URL; acute if rise and/or fall pattern present.
Acute MI: Acute myocardial injury + clinical evidence of ischemia + at least one of:
- Symptoms of ischemia
- New ischemic ECG changes
- Development of pathologic Q waves
- Imaging evidence of new loss of viable myocardium/RWMA
- Coronary thrombus on angiography or autopsy
MI Types
| Type | Mechanism |
|---|---|
| Type 1 | Atherothrombotic (plaque rupture/erosion) |
| Type 2 | Supply-demand imbalance (non-thrombotic) |
| Type 3 | Cardiac death before biomarkers available |
| Type 4a | PCI-related (cTn >5× 99th percentile URL) |
| Type 4b | Stent thrombosis |
| Type 5 | CABG-related (cTn >10× 99th percentile URL) |
Harrison's, p. 2161
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025), McGraw Hill Medical — Chapters 284 (Ischemic Heart Disease), 285 (Non-ST-Segment Elevation ACS), 286 (STEMI)
This is a shared conversation. Sign in to Orris to start your own chat.