Make a case study on coronary artery disease
Reading File
Finding Sources
Finding Sources
Searching PubMed
"coronary artery disease" AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Case Study: Coronary Artery Disease (CAD)
Patient Presentation
Patient: Mr. D.K., 58-year-old male
Chief Complaint: Recurrent, pressure-like chest pain radiating to the left arm and jaw for the past 3 weeks, now occurring at rest for 45 minutes.
History of Present Illness:
Mr. D.K. has had exertional chest pressure for the past 6 months, which he attributed to "stress." Over the past 3 weeks, episodes have increased in frequency, duration, and now occur at rest - a pattern shift suggesting progression from stable to unstable angina. Today's episode lasted 45 minutes and was accompanied by diaphoresis, nausea, and mild dyspnea. He denies syncope or palpitations.
Past Medical History:
- Type 2 diabetes mellitus (12 years, on metformin)
- Hypertension (8 years, on amlodipine)
- Hyperlipidemia (diagnosed incidentally 3 years ago, untreated)
- Current smoker - 30 pack-years
Family History: Father died of a heart attack at age 52. Maternal uncle with "heart problems."
Social History: Sedentary desk job, high-fat diet, BMI 29.4 (overweight), occasional alcohol use.
Review of Systems: Denies fever, weight loss, hemoptysis, cough, or leg swelling.
Physical Examination
| Parameter | Finding |
|---|---|
| BP | 158/96 mmHg |
| HR | 94 bpm, regular |
| RR | 18 breaths/min |
| SpO2 | 96% on room air |
| Temperature | 37.1°C |
| BMI | 29.4 |
Cardiovascular: Mild tachycardia; no murmurs, rubs, or gallops detected. No JVD. Peripheral pulses symmetric.
Respiratory: Clear to auscultation bilaterally, no crackles.
Abdomen: Soft, non-tender, no organomegaly.
Extremities: No peripheral edema. No xanthomas noted.
Background: Disease Overview
Definition
Coronary artery disease (CAD), also called ischemic heart disease (IHD), is the most common cause of mortality worldwide. It results from atherosclerotic obstruction of coronary arteries, creating an imbalance between myocardial oxygen supply and demand. This presents across a clinical spectrum ranging from stable angina to acute coronary syndromes (ACS). - Lippincott Illustrated Reviews: Pharmacology, p. 412
Epidemiology
Atherosclerosis and IHD have been correlated with multiple risk factors in prospective analyses, including the landmark Framingham Heart Study. These risk factors are roughly multiplicative in effect: two risk factors increase MI risk approximately 4-fold, and three factors (hyperlipidemia, hypertension, smoking) increase the rate by a factor of 7. - Robbins & Kumar Basic Pathology, p. [Table 8.2]
Pathophysiology
Atherosclerotic Plaque Formation
The underlying lesion of CAD is the atherosclerotic plaque. The process begins with endothelial dysfunction (from hypertension, dyslipidemia, smoking, or hyperglycemia), followed by:
- Lipid accumulation: LDL particles enter the subendothelial space and are oxidized. High LDL ("bad cholesterol") distributes cholesterol to peripheral tissues; HDL is protective by absorbing cholesterol from arterial walls. - Guyton & Hall Textbook of Medical Physiology
- Inflammatory response: Monocytes migrate in and differentiate into macrophages, engulfing oxidized LDL to form foam cells. Growth of atheroma is fueled by leukocyte trafficking and plaque hemorrhage.
- Fibrous cap formation: A fibrous cap overlies the lipid-rich necrotic core. Stable plaques have thick caps; vulnerable plaques have thin caps prone to rupture.
- Plaque rupture: Erosion or rupture of a vulnerable plaque exposes subendothelial proteins. Circulating platelets adhere, change shape, release thromboxane/ADP/fibrinogen, and activate GPIIb/IIIa receptors. Fibrinogen cross-links adjacent platelets, forming a platelet plug. Thrombin is then generated, converts fibrinogen to fibrin, and creates a platelet-rich thrombus. - Goldman-Cecil Medicine, p. 641
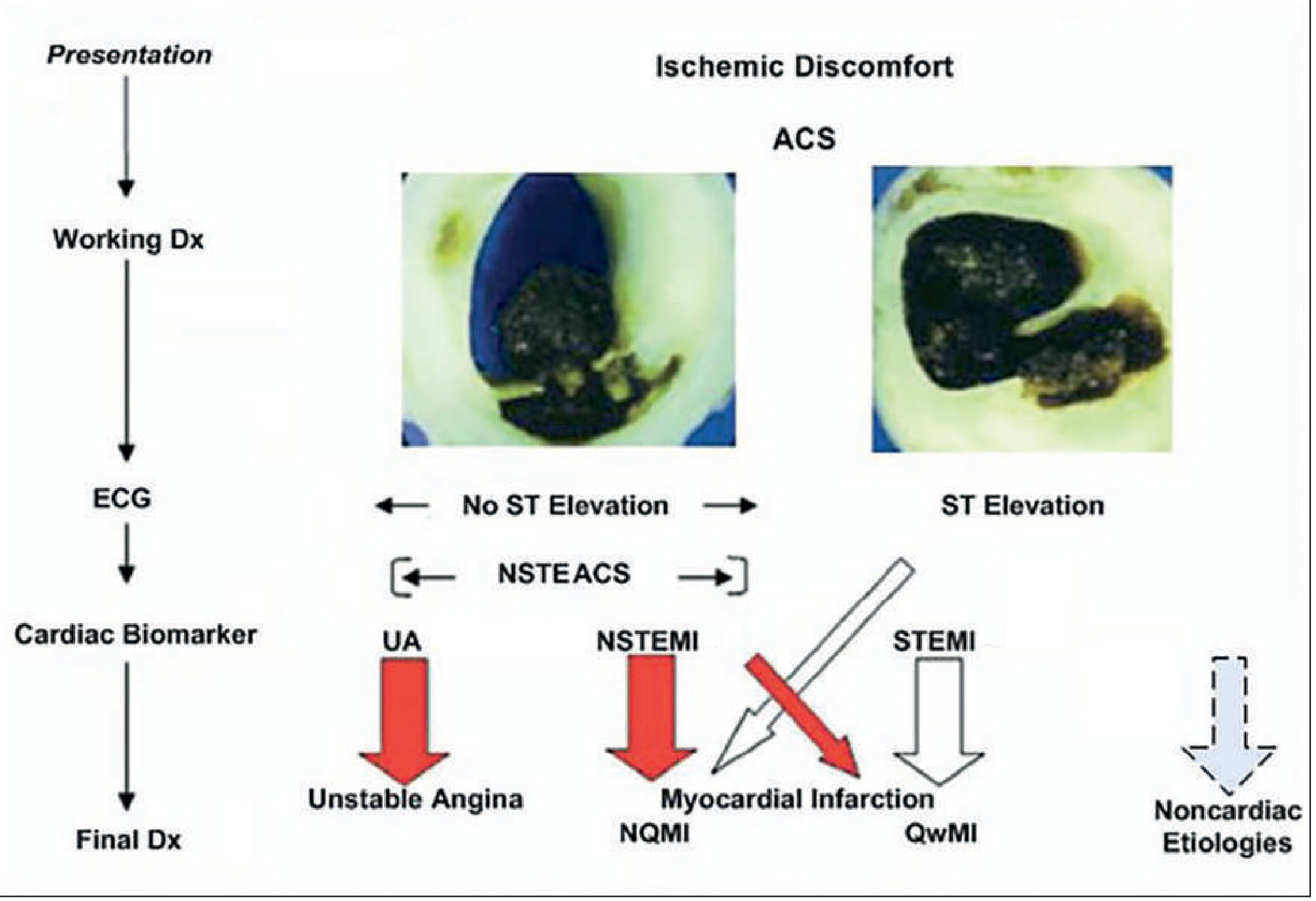
Ischemia Cascade
- Subtotal occlusion → transient ischemia without myonecrosis = Unstable Angina
- Subtotal occlusion + elevated troponin = NSTEMI (non-Q wave MI predominantly)
- Total occlusion → ST elevation on ECG → necrosis = STEMI (Q wave MI)
Risk Factors (This Patient)
Non-modifiable
| Factor | Presence in Mr. D.K. |
|---|---|
| Male sex | Yes |
| Age >40 years | Yes (58) |
| Family history | Yes (father MI at 52) |
Modifiable
| Factor | Status | Notes |
|---|---|---|
| Hypertension | Active | Increases CAD risk ≥2-fold alone |
| Diabetes mellitus | Active | >2-fold increased risk; with HTN = 8-fold risk |
| Hyperlipidemia | Untreated | LDL-driven, sufficient to cause lesions independently |
| Cigarette smoking | Active (30 pk-yr) | Direct endothelial toxin |
| Physical inactivity + overweight | Present | BMI 29.4 |
When hypertension, diabetes, and hyperlipidemia are all present together, the risk for atherosclerotic coronary artery disease is increased almost 20-fold. - Guyton & Hall Textbook of Medical Physiology
Diagnostic Workup
Electrocardiogram (ECG)
Findings in Mr. D.K.: ST segment depression of 1.5 mm in leads V4-V6, T-wave inversions in leads I, aVL - consistent with lateral wall ischemia (NSTEMI pattern).
- STEMI = ST elevation ≥1 mm in ≥2 contiguous leads, or new LBBB
- NSTEMI/UA = ST depression, T-wave inversion, or non-diagnostic ECG with biomarker elevation
- Myocardial ischemia is highly likely when anginal symptoms are accompanied by ECG abnormalities (Q waves, ST depression or elevation ≥1 mm, T-wave inversion in multiple precordial leads). - Goldman-Cecil Medicine, p. 641-642
Cardiac Biomarkers
| Biomarker | Finding | Interpretation |
|---|---|---|
| Troponin I (hs-cTnI) | Elevated at 0h and 3h | Confirms myocardial necrosis |
| CK-MB | Mildly elevated | Supportive |
| BNP | Mildly elevated | Suggests early LV strain |
The presence of elevated serum troponin distinguishes NSTEMI from unstable angina. - Goldman-Cecil Medicine
Additional Testing
The following diagnostic modalities are used in CAD evaluation per Sabiston Textbook of Surgery:
| Test | Purpose |
|---|---|
| Chest radiograph | Exclude pulmonary edema, cardiomegaly, aortic dissection |
| Transthoracic echocardiography (TTE) | Assess wall motion abnormalities, LV function (EF), valvular disease |
| Coronary CT angiography (CCTA) | Non-invasive visualization of coronary stenoses; excellent negative predictive value |
| Stress testing (exercise/pharmacologic) | Functional ischemia assessment in stable patients |
| Diagnostic cardiac catheterization | Gold standard - defines anatomy, stenosis severity; allows FFR/iFR measurement |
| FFR / iFR / OCT / IVUS | Intracoronary hemodynamic and anatomic assessment |
| SYNTAX score | Guides PCI vs. CABG decision in multivessel disease |
In Mr. D.K.: Given active NSTEMI presentation, urgent coronary angiography was performed, revealing:
- 85% stenosis in the proximal LAD (left anterior descending artery)
- 70% stenosis in the proximal RCA (right coronary artery)
- LVEF 50% (mildly reduced)
ACS Classification (Fourth Universal Definition)
| Type | Mechanism |
|---|---|
| Type 1 | Spontaneous plaque rupture/erosion with thrombus |
| Type 2 | Ischemic imbalance (e.g., demand ischemia from tachyarrhythmia, severe anemia) |
| Type 3 | Sudden cardiac death before biomarker results available |
| Type 4 | PCI-related MI |
| Type 5 | CABG-related MI |
Mr. D.K. = Type 1 NSTEMI. - Sabiston Textbook of Surgery
Risk Stratification
TIMI Score for UA/NSTEMI (Mr. D.K. scores 5/7 - High Risk):
- Age ≥65: No (1 pt)
- ≥3 CAD risk factors: Yes (1 pt) - diabetes, HTN, hyperlipidemia, smoking, family history
- Known CAD (stenosis ≥50%): Yes (1 pt)
- ST deviation ≥0.5 mm: Yes (1 pt)
- ≥2 anginal events in 24h: Yes (1 pt)
- Aspirin use in past 7 days: No
- Elevated cardiac markers: Yes (1 pt)
GRACE Score: Also calculated (incorporates age, heart rate, systolic BP, Killip class, creatinine, cardiac arrest, ST deviation, biomarkers). GRACE available at outcomes-umassmed.org/grace. - Goldman-Cecil Medicine
Differential Diagnosis
| Diagnosis | Key Distinguishing Features |
|---|---|
| NSTEMI (Working Dx) | Troponin rise, ST changes, typical pain, risk factors |
| Unstable Angina | Troponin negative |
| STEMI | ST elevation or new LBBB |
| Aortic Dissection | BP differential between arms, "tearing" pain to back |
| Pulmonary Embolism | Pleuritic pain, dyspnea, hypoxia, D-dimer elevation |
| Pericarditis | Friction rub, positional/pleuritic pain, diffuse ST elevation |
| Costochondritis | Reproducible tenderness on sternal palpation |
| GERD / esophageal spasm | Relief with antacids, no ECG changes |
Management
Immediate (Emergency)
MONA-B Protocol:
| Intervention | Rationale |
|---|---|
| Morphine (cautious use) | Analgesic, reduces anxiety/catecholamines |
| Oxygen | Maintain SpO2 ≥94% |
| Nitrates (sublingual/IV nitroglycerin) | Venodilation → reduces preload and myocardial O2 demand |
| Aspirin 325 mg (loading) | Irreversible COX-1 inhibition → reduces TXA2-mediated platelet aggregation |
| Beta-blocker | Reduces HR and myocardial O2 demand (IV metoprolol acutely, oral thereafter) |
Antiplatelet and Antithrombotic Therapy
The goals of treatment of non-ST elevation ACS are to prevent recurrent ischemia, prevent thrombus propagation, and stabilize the vulnerable plaque. - Goldman-Cecil Medicine, p. [treatment section]
| Agent | Mechanism | Notes |
|---|---|---|
| Aspirin | COX-1 inhibitor, reduces TXA2 | Lifelong therapy |
| P2Y12 inhibitor (ticagrelor, prasugrel, or clopidogrel) | Blocks ADP-mediated platelet activation | Dual antiplatelet therapy (DAPT) for 12 months post-ACS |
| UFH / LMWH (enoxaparin) | Thrombin/factor Xa inhibition | Short-term peri-procedural anticoagulation |
| GPIIb/IIIa inhibitors (tirofiban, eptifibatide) | Block fibrinogen cross-linking of platelets | High-risk/PCI patients |
A 2025 individual patient data meta-analysis in The Lancet (PMID: 40902613) found that clopidogrel may be comparable to aspirin for secondary prevention in some CAD patients - an important evolving evidence update.
Revascularization
PCI (Percutaneous Coronary Intervention):
- Preferred for NSTEMI/STEMI when technically feasible
- Recommended within 24-48 hours for high-risk NSTEMI
- Stent placement (drug-eluting stents preferred) restores coronary flow
CABG (Coronary Artery Bypass Grafting):
- Preferred over PCI in: left main disease, 3-vessel disease, diabetic patients with multivessel disease (FREEDOM trial)
- CABG reduces symptoms, cardiovascular events, and mortality in diabetic patients with extensive multivessel CAD. - Goldman-Cecil Medicine
In Mr. D.K.: Given 2-vessel disease and diabetes, a Heart Team discussion was held. PCI to the proximal LAD with a drug-eluting stent was performed successfully (TIMI 3 flow restored). The RCA lesion will be staged.
Guideline-Directed Medical Therapy (GDMT)
| Drug Class | Agent | Mechanism/Goal |
|---|---|---|
| Beta-blocker | Metoprolol succinate | Reduces HR, O2 demand, post-MI mortality |
| ACE inhibitor / ARB | Ramipril | Reduces afterload, prevents LV remodeling |
| Statin (high-intensity) | Rosuvastatin 40 mg | LDL lowering, plaque stabilization, anti-inflammatory |
| Antiplatelet (DAPT) | Aspirin + ticagrelor | Prevent stent thrombosis, recurrent ACS |
| Nitrate (as needed) | Sublingual nitroglycerin | Acute angina relief |
All patients with IHD should receive guideline-directed medical therapy with emphasis on lifestyle modifications (smoking cessation, physical activity, weight management) and management of modifiable risk factors (hypertension, diabetes, dyslipidemia). - Lippincott Illustrated Reviews: Pharmacology, p. 412
Medications for stable angina:
- Beta-blockers (metoprolol, bisoprolol, atenolol) - first-line; reduce HR and contractility
- Calcium channel blockers - dihydropyridines (amlodipine) for vasodilation; non-DHP (diltiazem, verapamil) for rate control
- Nitrates - nitroglycerin (sublingual, transdermal), isosorbide mono/dinitrate (long-acting)
- Ranolazine - sodium channel blocker; late INa inhibition reduces diastolic tension and O2 demand; useful as add-on therapy
- Lippincott Illustrated Reviews: Pharmacology
Complications
| Complication | Notes |
|---|---|
| Left ventricular dysfunction/failure | Most common serious complication |
| Ventricular arrhythmias (VF/VT) | Leading cause of sudden cardiac death post-MI |
| Mechanical complications | LV pseudoaneurysm, ventricular septal defect (VSD), papillary muscle rupture with mitral regurgitation |
| Cardiogenic shock | ~5-10% of STEMI; high mortality |
| Reinfarction / stent thrombosis | Reason for mandatory DAPT |
| Pericarditis (Dressler's syndrome) | Autoimmune; 1-8 weeks post-MI |
| Heart failure (chronic) | Long-term remodeling |
Sabiston Textbook of Surgery enumerates these mechanical complications as specific surgical indications.
Cardiac Rehabilitation and Secondary Prevention
| Component | Goal |
|---|---|
| Smoking cessation | Single most impactful modifiable intervention |
| Supervised exercise program | Improves functional capacity, reduces mortality |
| Dietary modification | Low saturated fat, Mediterranean-pattern diet |
| Weight management | BMI target <25 |
| BP control | Target <130/80 mmHg |
| Diabetes management | HbA1c <7%; SGLT2 inhibitors/GLP-1 agonists for CV benefit |
| Lipid management | LDL target <55 mg/dL (very high risk); high-intensity statin +/- ezetimibe/PCSK9i |
| Psychosocial support | Depression screening and treatment; a 2025 systematic review in the European Heart Journal (PMID: 40878995) highlights that depression in CAD is under-addressed in guidelines |
Hospital Course and Outcome
Mr. D.K. was admitted to the cardiac care unit, placed on DAPT (aspirin + ticagrelor), anticoagulated with enoxaparin, and underwent urgent PCI with drug-eluting stent placement to the proximal LAD within 24 hours. Post-procedure TIMI 3 flow was restored. Echo at discharge showed LVEF recovery to 55%. He was discharged on day 4 with:
- Aspirin 81 mg daily (lifelong)
- Ticagrelor 90 mg BD (12 months)
- Metoprolol succinate 50 mg daily
- Ramipril 5 mg daily
- Rosuvastatin 40 mg nightly
- Sublingual nitroglycerin (PRN)
- Metformin continued; endocrinology referral placed
- Cardiac rehab enrollment
- Smoking cessation counseling + varenicline prescription
Key Learning Points
- CAD is atherosclerosis-driven - endothelial injury, lipid deposition, inflammation, and plaque rupture lead to thrombus formation and ischemia.
- Risk factors are multiplicative: The combination of hypertension + diabetes + hyperlipidemia increases CAD risk ~20-fold. - Guyton & Hall
- ACS spectrum is defined by ECG (ST elevation vs. no ST elevation) and troponin (elevated vs. negative), distinguishing STEMI, NSTEMI, and UA.
- High-risk NSTEMI requires early invasive strategy (PCI within 24-48h); STEMI requires primary PCI within 90 minutes (door-to-balloon time).
- GDMT is mandatory post-ACS: DAPT, beta-blocker, ACE-inhibitor, high-intensity statin, with aggressive lifestyle modification.
- CABG is preferred over PCI in diabetic patients with multivessel disease and in left main disease.
- Secondary prevention must address all modifiable risk factors to prevent recurrence.
Sources:
- Goldman-Cecil Medicine, International Edition (2 Volume Set) - Chapter 57
- Robbins & Kumar Basic Pathology - Chapter 8
- Guyton & Hall Textbook of Medical Physiology - Chapter on Coronary Physiology
- Lippincott Illustrated Reviews: Pharmacology - Chapter 12 (IHD)
- Sabiston Textbook of Surgery - Chapter on Coronary Artery Disease and CABG
- Valgimigli M et al. Clopidogrel versus aspirin for secondary prevention of CAD. Lancet, 2025. PMID: 40902613
- Blatch Armon D et al. Depression and cardiovascular disease. Eur Heart J, 2025. PMID: 40878995










+16 more
Make on this patient
analyse_media
analyse_media
analyse_media
analyse_media
All data extracted. Now I have the complete picture from all 10 documents. Let me compile the full case study based on the real patient records.
Case Study: Coronary Artery Disease - Triple Vessel Disease (CAD-TVD)
Geetanjali Medical College & Hospital, Udaipur (Rajasthan)
Department of Cardiology | Radial Lounge
Primary Consultant: Dr. Ramesh Patel (DM Cardiology, PGIMER Chandigarh; FACC, FSCAI USA; Professor & HOD, Cardiology, GMCH)
1. Patient Identification
| Parameter | Details |
|---|---|
| Name | Mr. Fakir Mohammad |
| Age / Sex | 63 Years 6 Months / Male |
| Date of Birth | 01/01/1963 |
| Address | Gosi Mohella, Pani Ki Tanki, Abu Road, Sirohi, Rajasthan |
| UHID | 6246620 |
| IPD No. | 1207687 |
| Admission Date | 13/07/2026 at 12:03 PM |
| Expected Discharge | 23/07/2026 |
| Ward / Bed | Radial Lounge / MDI003 |
| Payer | AB Scheme - Maa Yojana |
2. Chief Complaints
- Shortness of Breath (SOB) - on exertion, NYHA Class II
- Chest pain on exertion - for 1-2 months (progressive)
3. History of Present Illness
Mr. Fakir Mohammad, a 63-year-old male with a known history of Coronary Artery Disease, Type 2 Diabetes Mellitus (T2DM), and Hypertension (HTN), presented to the Cardiology OPD on 13/07/2026 with a 1-2 month history of progressively worsening exertional chest pain and dyspnea on exertion (DOE Class II). He was already on cardiac medications including anti-anginals, antiplatelets, statins, and antidiabetics.
Given the worsening symptom burden despite medical therapy, he was advised admission for coronary angiography (CAG) in the Radial Lounge to reassess coronary anatomy and plan further intervention.
4. Past History (Relevant and Significant)
| Condition | Details |
|---|---|
| Hypertension (HTN) | Known, on treatment |
| Type 2 Diabetes Mellitus (T2DM) | Known, on antidiabetic therapy |
| CAD - Anterior Wall MI (AWMI) | Prior myocardial infarction - anterior wall |
| P/PCI to LM-LAD | Previous PCI to Left Main and LAD in 2016 |
| P/PCI to LAD | Repeat PCI to LAD on 18/02/2025 |
| EF ~35-40% | Chronically reduced ejection fraction |
| Antipsychotic medication | On medication for sleep disturbance/psychiatric co-morbidity |
| No H/o | Tuberculosis, Thyroid disease, Blood disorders (Bronchial Asthma) |
Clinical note: This patient has had three PCI procedures (LM-LAD 2016, LAD Feb 2025, and now planned LAD + RCA). His progressive disease despite prior revascularization is consistent with in-stent restenosis and advancing native vessel atherosclerosis in the setting of inadequately controlled risk factors.
5. Personal History
| Parameter | Details |
|---|---|
| Tobacco use | H/o chewing tobacco (significant risk factor) |
| Alcohol | No history |
| Smoking | No history |
| Sleep | Disturbed (on antipsychotic/sleep medication) |
| Appetite | Normal |
| Bladder / Bowel | Normal |
Family History: Not significant (N/S)
6. General Physical Examination
| Parameter | 13/07/2026 | 14/07/2026 (AM) | 15/07/2026 (AM) |
|---|---|---|---|
| BP | 120/69 mmHg | 135/70 mmHg | 121/61 mmHg |
| Pulse | 79 bpm | 97 bpm | 70/min |
| RR | 20/min | 20/min | 20/min |
| SpO2 | - | 94% on RA | 96% |
| Temperature | Afebrile | Afebrile | Afebrile |
General: No anemia, no cyanosis, no jaundice, no pedal edema, no clubbing, no lymphadenopathy, thyroid normal.
7. Systemic Examination
| System | Findings |
|---|---|
| CNS | Conscious and oriented |
| CVS | S1 S2 heard, no added sounds documented |
| Respiratory | Bilateral air entry present; bilateral lungs clear (no crackles) |
| Abdomen | Soft, non-tender |
8. Investigations
8A. Echocardiography (13/07/2026)
| Parameter | Value |
|---|---|
| LVIDd | 5.2 cm (dilated) |
| LVIDs | 4.0 cm |
| LV End-Diastolic Volume | 133 mL |
| LV End-Systolic Volume | 70 mL |
| IVSd | 1.4 cm (thickened) |
| PWd | 1.3 cm (thickened) |
| Left Atrium | 3.3 cm |
| Aortic root | 2.9 cm |
| LVEF (Visual) | 40-45% |
Echo Impression:
- CAD with Regional Wall Motion Abnormality (RWMA+)
- Hypokinesia involving apical septum and apex - consistent with prior anterior wall MI territory
- Moderate LV systolic dysfunction; LVEF ~40-45%
- Grade I LV diastolic dysfunction
- Concentric LVH (IVSd 1.4 cm, PWd 1.3 cm - from chronic hypertension)
- IAS/IVS intact; no vegetation or intra-cardiac masses
Clinical significance: LVEF 40-45% places this patient in the category of HFmrEF (Heart Failure with mildly reduced Ejection Fraction). The concentric LVH reflects long-standing hypertension, while the apical hypokinesia reflects the sequela of his prior anterior MI. This makes him high-risk for arrhythmias and worsening heart failure.
8B. Lab Investigations (Ordered)
Per progress notes, the following were ordered:
- CBC (Complete Blood Count) - Hb 8.20 g/dL noted (significant anemia)
- TLC - 6.88 × 10³/µL
- KFT (Kidney Function Tests) - serum creatinine
- LFT (Liver Function Tests)
- HbA1c (glycemic control assessment)
- CBT (Clotting / Bleeding Time)
- Chest X-Ray (CXR)
Anemia (Hb 8.20 g/dL) is a significant co-morbidity in this patient. It increases myocardial oxygen demand (type 2 MI mechanism), worsens angina, and is a bleeding risk factor with antiplatelet therapy. The team noted: "Arrange 10 PRBC" (arrange 10 units packed red blood cells - or likely 1 unit PRBC transfusion was planned).
8C. Coronary Angiography Report (13/07/2026)
- Institution: GMCH, Dept. of Cardiology
- Access: Right Radial Artery
- Catheter: 5 Fr Tiger
- Dye: Omnipaque
- Aortic pressure: 120/70 mmHg
- Consultant team: Dr. Ramesh Patel, Dr. Dilip Jain, Dr. Gaurav Mittal, Dr. Rohin K. Saini
| Vessel | Findings |
|---|---|
| Left Main (LM) | Patent stent (from 2016 PCI) with plaque+ |
| Left Anterior Descending (LAD) | Type III; mid 80-90% disease; patent stent (from Feb 2025 PCI) |
| Left Circumflex (LCx) | Chronic Total Occlusion (CTO) with retrograde supply from RCA |
| Right Coronary Artery (RCA) | Dominant; proximal 70-80% stenosis |
Impression: CAD - Triple Vessel Disease (CAD-TVD)
Advice: PCI to LAD and RCA
Anatomy summary: This is complex, high-risk anatomy. The LCx CTO receiving collateral supply from RCA means the RCA is currently providing retrograde perfusion to an entire LCx territory on top of its own. Treating the RCA with PCI (removing the 70-80% obstruction) will restore antegrade flow and protect both the RCA and LCx territories.
9. Diagnosis (Final / Working)
| # | Diagnosis |
|---|---|
| 1 | CAD - Triple Vessel Disease (CAD-TVD) |
| 2 | Prior AWMI (Anterior Wall Myocardial Infarction) |
| 3 | Post PCI to LM-LAD (2016) |
| 4 | Post PCI to LAD (18/02/2025) |
| 5 | Moderate LV Systolic Dysfunction (LVEF 40-45%) |
| 6 | Type 2 Diabetes Mellitus (T2DM) |
| 7 | Hypertension (HTN) |
| 8 | Symptomatic Anemia (Hb 8.2 g/dL) |
10. Progress Notes Summary
| Date | Vitals | Plan |
|---|---|---|
| 13/07/2026 (Eve) | BP 135/70, P 97, RR 20, SpO2 94% RA | CAG done. Findings: CAD-TVD. Plan: PCI to LAD + RCA. CNS examination - normal |
| 14/07/2026 (AM) | BP 130/68, HR 68, RR 16, Temp afebrile, SpO2 94% RA | Advise: CBC, KFT, LFT, HbA1c. Arrange PRBC. Plan: PCI to LAD + RCA |
| 15/07/2026 (AM) | BP 121/61, HR 70, RR 20, SpO2 96% | CBT, CBC, KFT, LFT, HbA1c. Plan: PCI to LAD + RCA |
11. Medications (Current - Prescribed 13/07/2026 by Dr. Ramesh Patel)
| # | Drug (Brand) | Composition | Dose | Timing | Rationale |
|---|---|---|---|---|---|
| 1 | Rozucor Gold 20mg | Aspirin 75mg + Clopidogrel 75mg + Rosuvastatin 20mg | 0-0-1 | 9 PM daily | DAPT (dual antiplatelet) + statin for CAD secondary prevention |
| 2 | Sitaxa DM 10/100/500mg | Dapagliflozin 10mg + Metformin 500mg + Sitagliptin 100mg | 0-1-0 | Before lunch | Triple antidiabetic; SGLT2i (dapagliflozin) adds cardiovascular mortality benefit in CAD + T2DM |
| 3 | Met XL R 25/2.5mg | Metoprolol 25mg + Ramipril 2.5mg | 1-0-0 | 9 AM | Beta-blocker (reduces HR/O2 demand) + ACEi (reduces LV remodeling, controls BP) |
| 4 | Renuca 500mg | Ranolazine 500mg | 1-0-1 | After breakfast + dinner | Anti-anginal (late INa inhibitor); reduces diastolic tension, relieves chronic angina |
| 5 | Monit GTN 2.6mg | Nitroglycerin 2.6mg (sustained release) | 1-1-0 | 8 AM + 4 PM | Nitrate for angina prophylaxis; reduces preload and O2 demand |
| 6 | Pantocid DSR | Pantoprazole 40mg + Domperidone 30mg | 1-0-0 | 7 AM | Gastroprotection (PPI) given dual antiplatelet therapy |
Pharmacology note: Dapagliflozin (SGLT2 inhibitor) in this patient is particularly important. In the DAPA-HF trial, dapagliflozin reduced cardiovascular death and worsening heart failure in patients with HFrEF/HFmrEF regardless of diabetes status. This patient's LVEF of 40-45% and T2DM make him a strong candidate. - Lippincott Illustrated Reviews: Pharmacology
12. Pathophysiology Applied to This Patient
Why Did the Disease Progress Despite Prior PCI?
-
In-stent restenosis / disease progression: The 2016 LM-LAD stent is patent but has plaque accumulation. The 2025 LAD stent is also patent but has developed mid-vessel 80-90% disease distal to it. This represents progressive native vessel disease.
-
Inadequately controlled risk factors: Ongoing T2DM, HTN, and tobacco chewing (a significant risk factor even without cigarette smoking - causes endothelial injury and platelet activation) drive continued atherosclerotic progression.
-
LCx CTO: Complete occlusion of the circumflex likely occurred gradually. Retrograde collateral supply from the dominant RCA is maintaining viability of the LCx territory - this is a protective mechanism (collateral circulation).
-
Reduced EF (35-45%): Result of the prior anterior wall MI (apical septum + apex hypokinesia on echo), representing permanent scar from the AWMI. The remaining viable but ischemic myocardium is at risk if the LAD disease and RCA stenosis are not treated.
-
Concentric LVH: Driven by long-standing hypertension. This reduces LV compliance (Grade I diastolic dysfunction), increases O2 demand, and worsens the supply-demand mismatch.
13. Planned Procedure: PCI to LAD and RCA
Indication: Symptomatic CAD (exertional chest pain + dyspnea) despite GDMT, with angiographically severe multivessel disease (LAD 80-90%, RCA 70-80%).
Approach: Right Radial Artery access (already used for diagnostic CAG - reduces bleeding risk vs. femoral access, allows early ambulation).
Procedural considerations:
- LAD PCI: Mid-vessel 80-90% lesion (Type III vessel). Likely requires drug-eluting stent (DES). Prior stent is patent - this is a new lesion.
- RCA PCI: Proximal 70-80% stenosis in a dominant RCA. Critical to treat - this vessel also supplies the LCx territory retrograde. Successful PCI will restore flow to two territories.
- LCx CTO: Not planned for intervention in this admission (complex; CTO PCI carries higher risk and requires specialized retrograde approach techniques).
Pre-procedure preparation:
- Ensure adequate antiplatelet loading (aspirin + clopidogrel already on board via Rozucor Gold)
- Correct anemia (Hb 8.2 - arrange PRBC transfusion pre-procedure to reduce type 2 ischemia risk)
- Optimize glycemic control (HbA1c pending)
- KFT / creatinine clearance - for contrast dosing (dye load calculation, risk of contrast nephropathy)
14. Key Learning Points from This Case
| # | Learning Point |
|---|---|
| 1 | CAD-TVD with prior AWMI represents an advanced, high-risk phenotype. Multiple prior PCIs do not prevent disease progression if underlying risk factors (DM, HTN, tobacco) are uncontrolled. |
| 2 | LCx CTO with retrograde collateral supply from RCA illustrates the importance of the dominant RCA in collateral circulation - treating the RCA stenosis protects two territories simultaneously. |
| 3 | LVEF 40-45% (HFmrEF) - Moderate LV dysfunction in this patient is irreversible (scar from AWMI) + potentially reversible (hibernating myocardium in ischemic zones). Successful revascularization may partially improve EF. |
| 4 | Concentric LVH + Grade I diastolic dysfunction from chronic hypertension co-exists with systolic dysfunction - a "double burden" on this heart. |
| 5 | Anemia (Hb 8.2 g/dL) is a type 2 MI trigger (increased demand, decreased supply) and must be corrected before intervention. It also increases bleeding risk on DAPT. |
| 6 | Tobacco chewing (without cigarette smoking) is a recognized independent cardiovascular risk factor - platelet activation, endothelial injury, and nicotine-mediated vasospasm. |
| 7 | Ranolazine is appropriately added for chronic angina refractory to nitrates and beta-blockers - late INa inhibition reduces diastolic wall tension and O2 consumption. |
| 8 | SGLT2 inhibitor (Dapagliflozin) in CAD + T2DM + reduced EF provides triple benefit: glycemic control, heart failure risk reduction, and renal protection. |
| 9 | Radial access for PCI reduces vascular complications vs. femoral access in a high-risk patient on DAPT. |
Hospital: Geetanjali Medical College & Hospital, Udaipur, Rajasthan
Consultant Team: Dr. Ramesh Patel (HOD Cardiology), Dr. Dilip Jain, Dr. Gaurav Mittal, Dr. Rohin K. Saini, Dr. Manisha Sir, Dr. Megha
This is a shared conversation. Sign in to Orris to start your own chat.